

Gray matter injury associated with periventricular leukomalacia in the premature infant
- PMID: 17912538
- PMCID: PMC2080348
- DOI: 10.1007/s00401-007-0295-5
Gray matter injury associated with periventricular leukomalacia in the premature infant
Abstract
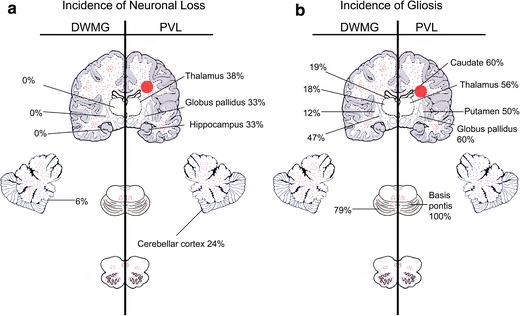
Neuroimaging studies indicate reduced volumes of certain gray matter regions in survivors of prematurity with periventricular leukomalacia (PVL). We hypothesized that subacute and/or chronic gray matter lesions are increased in incidence and severity in PVL cases compared to non-PVL cases at autopsy. Forty-one cases of premature infants were divided based on cerebral white matter histology: PVL (n = 17) with cerebral white matter gliosis and focal periventricular necrosis; diffuse white matter gliosis (DWMG) (n = 17) without necrosis; and "Negative" group (n = 7) with no abnormalities. Neuronal loss was found almost exclusively in PVL, with significantly increased incidence and severity in the thalamus (38%), globus pallidus (33%), and cerebellar dentate nucleus (29%) compared to DWMG cases. The incidence of gliosis was significantly increased in PVL compared to DWMG cases in the deep gray nuclei (thalamus/basal ganglia; 50-60% of PVL cases), and basis pontis (100% of PVL cases). Thalamic and basal ganglionic lesions occur almost exclusively in infants with PVL. Gray matter lesions occur in a third or more of PVL cases suggesting that white matter injury generally does not occur in isolation, and that the term "perinatal panencephalopathy" may better describe the scope of the neuropathology.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PMC', 'value': 'PMC1648870', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1648870/'}, {'type': 'PubMed', 'value': '4834016', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/4834016/'}]}
- Armstrong D, Norman MG (1974) Periventricular leucomalacia in neonates. Complications and sequelae. Arch Dis Child 49:367–375 - PMC - PubMed
-
- None
- Auer RN, Sutherland GR (2002) Hypoxia and related conditions. In: Graham DI, Lantos PL (eds) Greenfield’s neuropathology, 7th edn. Arnold, London, pp 234–280
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '11853021', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11853021/'}]}
- Back SA, Luo NL, Borenstein NS, Volpe JJ, Kinney HC (2002) Arrested oligodendrocyte lineage progression during human cerebral white matter development: dissociation between the timing of progenitor differentiation and myelinogenesis. J Neuropathol Exp Neurol 61:197–211 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '13966380', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/13966380/'}]}
- Banker BQ, Larroche JC (1962) Periventricular leukomalacia of infancy. A form of neonatal anoxic encephalopathy. Arch Neurol 7:386–410 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1093/brain/awh436', 'is_inner': False, 'url': 'https://doi.org/10.1093/brain/awh436'}, {'type': 'PubMed', 'value': '15705606', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15705606/'}]}
- Bell JE, Becher JC, Wyatt B, Keeling JW, McIntosh N (2005) Brain damage and axonal injury in a Scottish cohort of neonatal deaths. Brain 128:1070–1081 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
