

Shared medical appointments based on the chronic care model: a quality improvement project to address the challenges of patients with diabetes with high cardiovascular risk
- PMID: 17913775
- PMCID: PMC2464960
- DOI: 10.1136/qshc.2006.019158
Shared medical appointments based on the chronic care model: a quality improvement project to address the challenges of patients with diabetes with high cardiovascular risk
Abstract
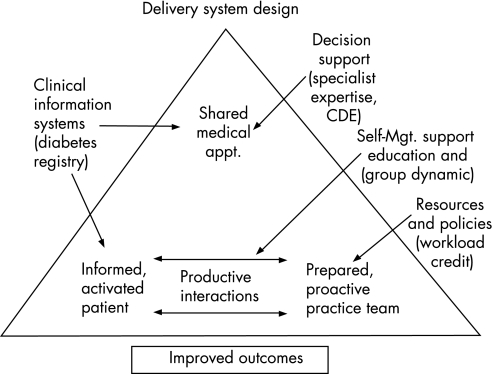
Objective: The epidemic proportions and management complexity of diabetes have prompted efforts to improve clinic throughput and efficiency. One method of system redesign based on the chronic care model is the Shared Medical Appointment (SMA) in which groups of patients (8-20) are seen by a multi-disciplinary team in a 1-2 h appointment. Evaluation of the impact of SMAs on quality of care has been limited. The purpose of this quality improvement project was to improve intermediate outcome measures for diabetes (A1c, SBP, LDL-cholesterol) focusing on those patients at highest cardiovascular risk.
Setting: Primary care clinic at a tertiary care academic medical center.
Subjects: Patients with diabetes with one or more of the following: A1c >9%, SBP blood pressure >160 mm Hg and LDL-c >130 mg/dl were targeted for potential participation; other patients were referred by their primary care providers. Patients participated in at least one SMA from 4/05 to 9/05.
Study design: Quasi-experimental with concurrent, but non-randomised controls (patients who participated in SMAs from 5/06 through 8/06; a retrospective period of observation prior to their SMA participation was used).
Intervention: SMA system redesign. ANALYTICAL METHODS: Paired and independent t tests, chi(2) tests and Fisher Exact tests.
Results: Each group had up to 8 patients. Patients participated in 1-7 visits. At the initial visit, 83.3% had A1c levels >9%, 30.6% had LDL-cholesterol levels >130 mg/dl, and 34.1% had SBP >or=160 mm Hg. Levels of A1c, LDL-c and SBP all fell significantly postintervention with a mean (95% CI) decrease of A1c 1.4 (0.8, 2.1) (p<0.001), LDL-c 14.8 (2.3, 27.4) (p = 0.022) and SBP 16.0 (9.7, 22.3) (p<0.001). There were no significant differences at baseline between control and intervention groups in terms of age, baseline intermediate outcomes, or medication use. The reductions in A1c in % and SBP were greater in the intervention group relative to the control group: 1.44 vs -0.30 (p = 0.002) for A1c and 14.83 vs 2.54 mm Hg (p = 0.04) for SBP. LDL-c reduction was also greater in the intervention group, 16.0 vs 5.37 mg/dl, but the difference was not statistically significant (p = 0.29).
Conclusions: We were able to initiate a programme of group visits in which participants achieved benefits in terms of cardiovascular risk reduction. Some barriers needed to be addressed, and the operations of SMAs evolved over time. Shared medical appointments for diabetes constitute a practical system redesign that may help to improve quality of care.
Conflict of interest statement
Competing interests: None declared.
Comment in
-
Diversifying the options for interacting with patients.Qual Saf Health Care. 2007 Oct;16(5):322-3. doi: 10.1136/qshc.2007.022970. Qual Saf Health Care. 2007. PMID: 17913770 Free PMC article.
Similar articles
-
Maintenance of Clinical Endpoints After Discharge from a Pharmacist-Managed Risk Reduction Clinic at a Veterans Affairs Medical Center.J Manag Care Spec Pharm. 2016 Jan;22(1):14-20. doi: 10.18553/jmcp.2016.22.1.14. J Manag Care Spec Pharm. 2016. PMID: 27015047 Free PMC article.
-
Shared Medical Appointments: Impact on Clinical and Quality Outcomes in Veterans With Diabetes.Qual Manag Health Care. 2016 Jul-Sep;25(3):176-80. doi: 10.1097/QMH.0000000000000098. Qual Manag Health Care. 2016. PMID: 27367218
-
Effect of a Collaborative Care Model on Depressive Symptoms and Glycated Hemoglobin, Blood Pressure, and Serum Cholesterol Among Patients With Depression and Diabetes in India: The INDEPENDENT Randomized Clinical Trial.JAMA. 2020 Aug 18;324(7):651-662. doi: 10.1001/jama.2020.11747. JAMA. 2020. PMID: 32809002 Free PMC article. Clinical Trial.
-
A Narrative Review of Diabetes Group Visits in Low-Income and Underserved Settings.Curr Diabetes Rev. 2019;15(5):372-381. doi: 10.2174/1573399814666181112145910. Curr Diabetes Rev. 2019. PMID: 30421682 Free PMC article. Review.
-
Multidisciplinary collaborative care in the management of patients with uncontrolled diabetes: A systematic review and meta-analysis.Int J Clin Pract. 2019 Feb;73(2):e13288. doi: 10.1111/ijcp.13288. Epub 2018 Nov 29. Int J Clin Pract. 2019. PMID: 30369012
Cited by
-
A randomized controlled trial of an internet-based mentoring program for type 1 diabetes patients with inadequate glycemic control.Diabetes Metab J. 2014 Apr;38(2):134-42. doi: 10.4093/dmj.2014.38.2.134. Epub 2014 Apr 18. Diabetes Metab J. 2014. PMID: 24851207 Free PMC article.
-
A realist review of shared medical appointments: How, for whom, and under what circumstances do they work?BMC Health Serv Res. 2017 Feb 4;17(1):113. doi: 10.1186/s12913-017-2064-z. BMC Health Serv Res. 2017. PMID: 28160771 Free PMC article. Review.
-
Quality improvement initiative for rapid induction of hypertension control in primary care.Circ Cardiovasc Qual Outcomes. 2010 Sep;3(5):558-64. doi: 10.1161/CIRCOUTCOMES.109.913137. Circ Cardiovasc Qual Outcomes. 2010. PMID: 20841550 Free PMC article. No abstract available.
-
The impact of interventions on appointment and clinical outcomes for individuals with diabetes: a systematic review.BMC Health Serv Res. 2015 Sep 2;15:355. doi: 10.1186/s12913-015-0938-5. BMC Health Serv Res. 2015. PMID: 26330299 Free PMC article.
-
Effect of Peer Mentors in Diabetes Self-management vs Usual Care on Outcomes in US Veterans With Type 2 Diabetes: A Randomized Clinical Trial.JAMA Netw Open. 2020 Sep 1;3(9):e2016369. doi: 10.1001/jamanetworkopen.2020.16369. JAMA Netw Open. 2020. PMID: 32915236 Free PMC article. Clinical Trial.
References
-
- King H, Aubert R, Herman H. Global burden of diabetes, 1995–2025: Prevalence, numerical estimates and projects. Diabetes Care 1997211414–1431. - PubMed
-
- Noffsinger E. Increasing quality care and access while reducing cost through drop‐in group medical appointments (DIGMAs). Group Pract J 19994812–18.
-
- Noffsinger E, Scott J. Understanding today's group visit models. Group Pract J 2000Feb46–58.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical