

A cost-effectiveness analysis of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in diabetic nephropathy
- PMID: 17917502
- PMCID: PMC8109938
- DOI: 10.1111/j.1524-6175.2007.07182.x
A cost-effectiveness analysis of angiotensin-converting enzyme inhibitors and angiotensin receptor blockers in diabetic nephropathy
Abstract
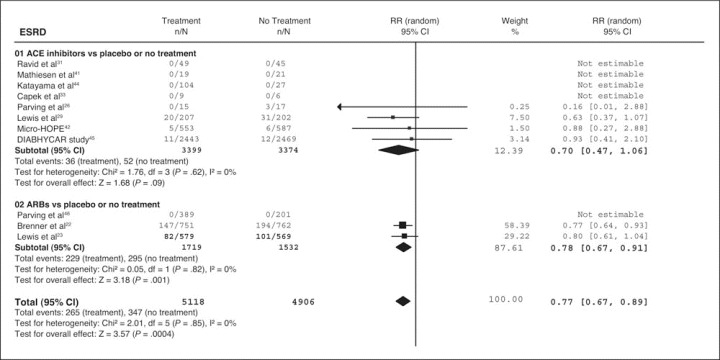
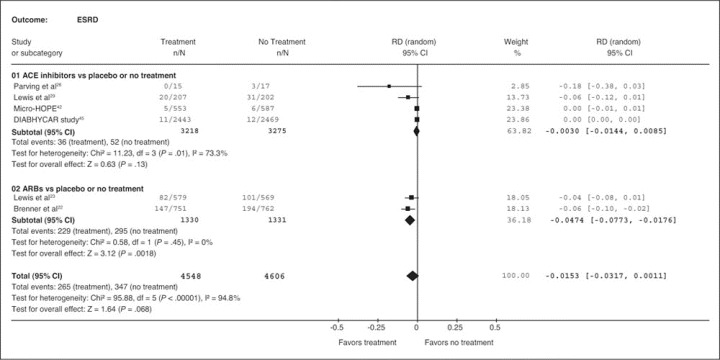
The aim of this study was to estimate the cost-effectiveness of renin-angiotensin-aldosterone system blockers in patients with diabetic nephropathy. A cost-effectiveness analysis was performed based on a meta-analysis of studies investigating the effect of angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) as part of a treatment regimen on the incidence of end-stage renal disease (ESRD) in patients with diabetic nephropathy. The primary outcome was the cost to prevent 1 patient from developing ESRD. Cost analysis was performed from a third-party payer perspective in 2006 US dollars. As part of a treatment regimen, ARBs significantly reduced the incidence of ESRD and doubling of serum creatinine concentration (P<.05) but not total mortality. The cost to prevent 1 patient from developing ESRD was $31,729 (95% confidence interval, $19,443-$85,442; P<.01), $189,190 (P=.13) and $51,585 (P=.068) for patients receiving ARBs, ACE inhibitors, or either of them, respectively. This study demonstrates that blocking the RAAS, which delays the progression to ESRD, appears to be cost-effective. The current analysis favors ARBs in terms of cost-effectiveness.
Figures
Similar articles
-
Effects of renin-angiotensin system blockers on renal outcomes and all-cause mortality in patients with diabetic nephropathy: an updated meta-analysis.Am J Hypertens. 2008 Aug;21(8):922-9. doi: 10.1038/ajh.2008.206. Epub 2008 Jun 5. Am J Hypertens. 2008. PMID: 18535536
-
Pharmacoeconomic challenges in the management of diabetic nephropathy.J Manag Care Pharm. 2004 Sep;10(5 Suppl A):S6-11. doi: 10.18553/jmcp.2004.10.S5-A.S6. J Manag Care Pharm. 2004. PMID: 15369419 Free PMC article.
-
Angiotensin-converting enzyme inhibitors versus angiotensin receptor blockers for diabetic nephropathy: a retrospective comparison.J Renin Angiotensin Aldosterone Syst. 2009 Dec;10(4):195-200. doi: 10.1177/1470320309352352. J Renin Angiotensin Aldosterone Syst. 2009. PMID: 20026868
-
Preventing end-stage renal disease in diabetic patients - dual blockade of the renin-angiotensin system (Part II).J Renin Angiotensin Aldosterone Syst. 2005 Sep;6(2):55-68. doi: 10.3317/jraas.2005.011. J Renin Angiotensin Aldosterone Syst. 2005. PMID: 16470484 Review.
-
The RAAS in the pathogenesis and treatment of diabetic nephropathy.Nat Rev Nephrol. 2010 Jun;6(6):319-30. doi: 10.1038/nrneph.2010.58. Epub 2010 May 4. Nat Rev Nephrol. 2010. PMID: 20440277 Review.
Cited by
-
Cost effectiveness of vildagliptin versus glimepiride as add-on treatment to metformin for the treatment of diabetes mellitus type 2 patients in Greece.Cost Eff Resour Alloc. 2017 Sep 6;15:19. doi: 10.1186/s12962-017-0082-7. eCollection 2017. Cost Eff Resour Alloc. 2017. PMID: 28904527 Free PMC article.
-
Effectiveness, safety and cost of drug substitution in hypertension.Br J Clin Pharmacol. 2010 Sep;70(3):320-34. doi: 10.1111/j.1365-2125.2010.03681.x. Br J Clin Pharmacol. 2010. PMID: 20716230 Free PMC article.
-
Phase 4 Studies in Heart Failure - What is Done and What is Needed?Curr Cardiol Rev. 2016;12(3):216-30. doi: 10.2174/1573403x12666160606121458. Curr Cardiol Rev. 2016. PMID: 27280303 Free PMC article. Review.
-
Angiotensin Receptor Blockers Versus Angiotensin Converting Enzyme Inhibitors for the Treatment of Arterial Hypertension and the Role of Olmesartan.Adv Ther. 2019 Feb;36(2):278-297. doi: 10.1007/s12325-018-0859-x. Epub 2018 Dec 27. Adv Ther. 2019. PMID: 30591990 Free PMC article. Review.
References
-
- Registry ERA‐EDTA. European Renal Association‐European Dialysis and Transplant Association Registry 2004 Annual Report. Amsterdam, the Netherlands: Academic Medical Center, Department of Medical Informatics; 2006.
-
- US Renal Data System. USRDS 2006 Annual Data Report: Atlas of End‐Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2006.
-
- Grassmann A, Gioberge S, Moeller S, et al. ESRD patients in 2004: global overview of patient numbers, treatment modalities and associated trends. Nephrol Dial Transplant. 2005;20(12):2587–2593. - PubMed
-
- Xue JL, Ma JZ, Louis TA, et al. Forecast of the number of patients with end‐stage renal disease in the United States to the year 2010. J Am Soc Nephrol. 2001;12(12):2753–2758. - PubMed
-
- Athyros VG, Bouloukos VI, Pehlivanidis AN, et al. The prevalence of the metabolic syndrome in Greece: The MetS‐Greece Multicentre Study. Diabetes Obes Metab. 2005;7(4):397–405. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
