

CD4/CD8 T-cell ratio predicts HIV infection in infants: the National Heart, Lung, and Blood Institute P2C2 Study
- PMID: 17920669
- PMCID: PMC4271194
- DOI: 10.1016/j.jaci.2007.08.037
CD4/CD8 T-cell ratio predicts HIV infection in infants: the National Heart, Lung, and Blood Institute P2C2 Study
Abstract
Background: In resource-poor regions of the world, HIV virologic testing is not available.
Objective: We sought to evaluate the diagnostic usefulness of the CD4/CD8 T-cell ratio in predicting HIV infection in infants.
Methods: Data from the 3- and 9-month visits for non-breast-fed infants born to HIV-infected mothers enrolled (1990-1994) in the Pediatric Pulmonary and Cardiac Complications of Vertically Transmitted HIV Infection Study (mother-to-child transmission of HIV, 17%) were analyzed. Data from the 3-month visit for infants enrolled (1985-1996) in the Perinatal AIDS Collaborative Transmission Study (mother-to-child transmission of HIV, 18%) were used for validation.
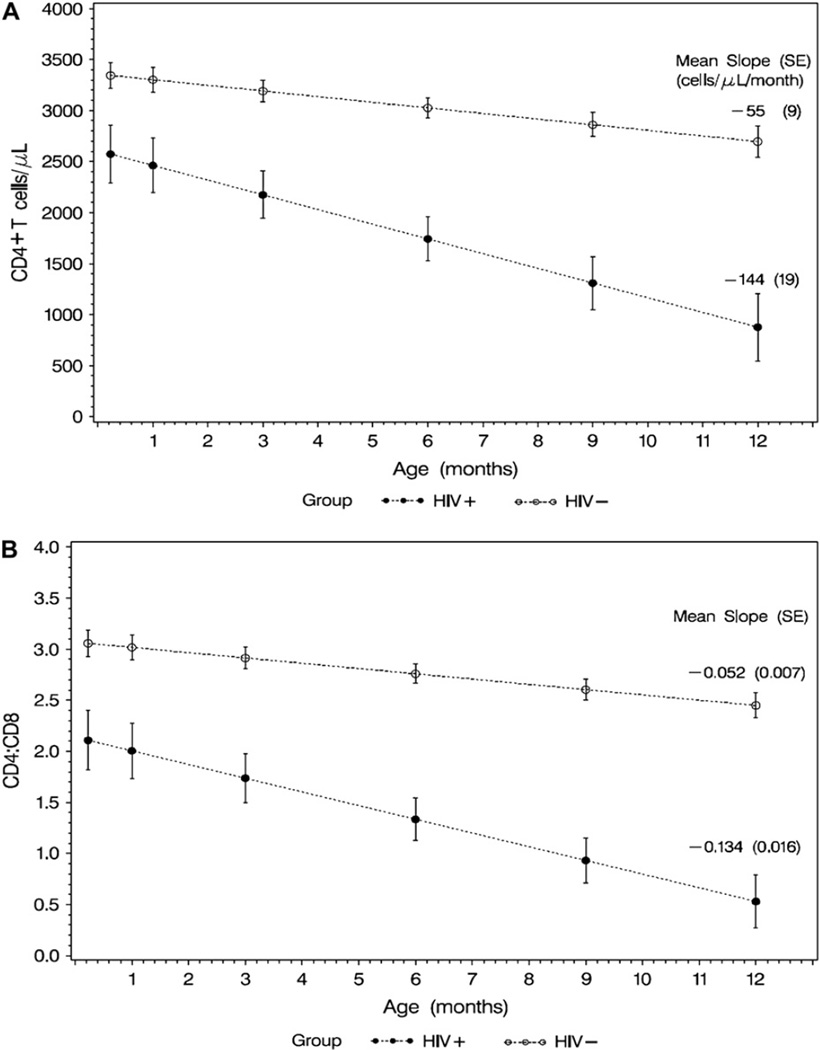
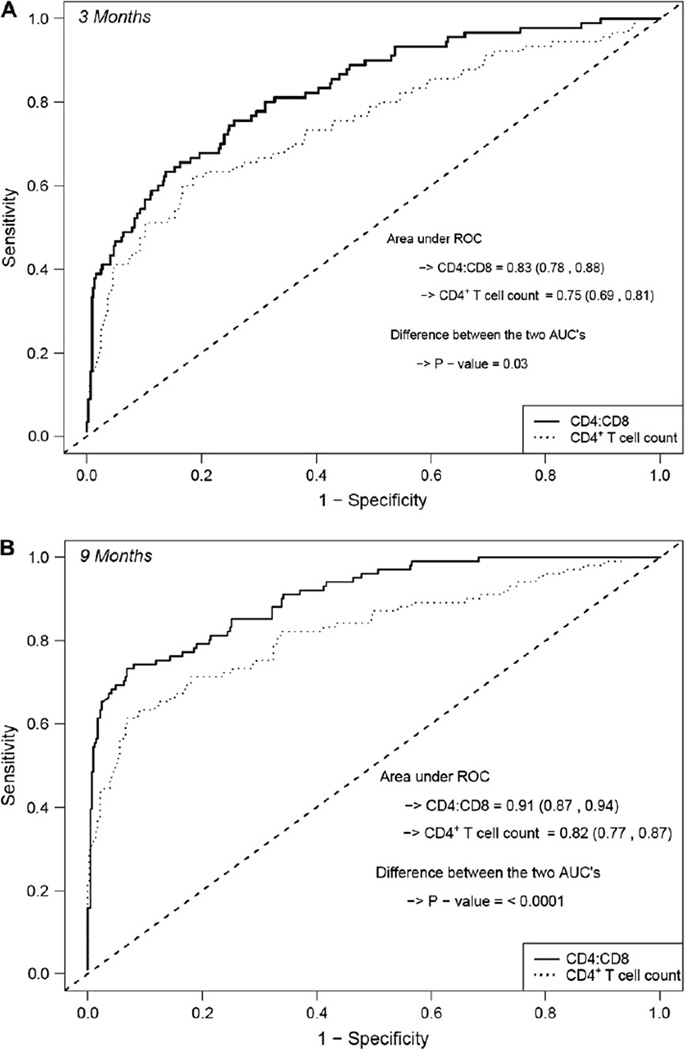
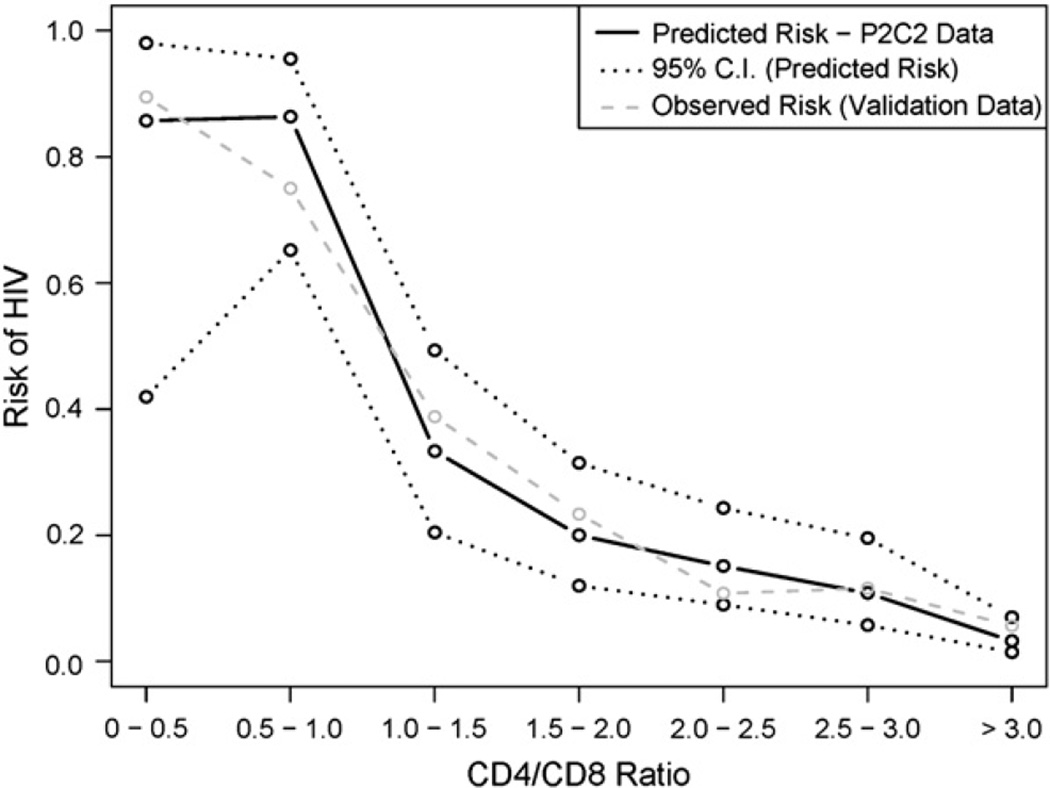
Results: At 3 months of age, data were available on 79 HIV-infected and 409 uninfected non-breast-fed infants in the Pediatric Pulmonary and Cardiac Complications of Vertically Transmitted HIV Infection Study. The area under the curve (AUC) of the receiver operating characteristic curve at 3 months was higher for the CD4/CD8 ratio compared with the CD4(+) T-cell count (AUC, 0.83 and 0.75; P = .03). The mean CD4/CD8 ratio at the 3-month visit was 1.7 for HIV-infected infants and 3.0 for uninfected infants. A CD4/CD8 ratio of 2.4 at 3 months of age was almost 2.5 times more likely to occur in an HIV-infected infant compared with an uninfected infant (test sensitivity, 81%; posttest probability of HIV, 33%). Model performance in the Centers for Disease Control and Prevention Perinatal AIDS Collaborative Transmission Study validation test (224 HIV-infected and 1015 uninfected 3-month-old infants) was equally good (AUC, 0.78 for CD4/CD8 ratio).
Conclusion: The CD4/CD8 T-cell ratio is a more sensitive predictor of HIV infection in infants than the CD4(+) T-cell count.
Clinical implications: The CD4/CD8 T-cell ratio can be used with caution to predict HIV infection in children.
Conflict of interest statement
Disclosure of potential conflict of interest: The authors have declared that they have no conflict of interest.
Figures
References
-
- Gortmaker SL, Hughes M, Cervia J, Brady M, Johnson GM, Seage GR., 3rd Effect of combination therapy including protease inhibitors on mortality among children and adolescents infected with HIV-1. N Engl J Med. 2001;345:1522–1528. - PubMed
-
- Gona P, Van Dyke RB, Williams PL, Dankner WM, Chernoff MC, Nachman SA, et al. Incidence of opportunistic and other infections in HIV-infected children in the HAART era. JAMA. 2006;296:292–300. - PubMed
-
- Palumbo P. Diagnostic methods for infants born to HIV-infected women. In: Shearer WT, Hanson IC, editors. Medical management of AIDS in children. Philadelphia: Elsevier/Saunders; 2003. pp. 107–116.
Publication types
MeSH terms
Grants and funding
- R01 HL079533/HL/NHLBI NIH HHS/United States
- N01 HR096037/HR/NHLBI NIH HHS/United States
- HL96040/HL/NHLBI NIH HHS/United States
- U01 AI027551/AI/NIAID NIH HHS/United States
- AI36211/AI/NIAID NIH HHS/United States
- AI27551/AI/NIAID NIH HHS/United States
- HD41983/HD/NICHD NIH HHS/United States
- P30 A1050409/PHS HHS/United States
- K01 RR000188/RR/NCRR NIH HHS/United States
- M01 RR000188/RR/NCRR NIH HHS/United States
- AI41089/AI/NIAID NIH HHS/United States
- P30 AI036211/AI/NIAID NIH HHS/United States
- RR0188/RR/NCRR NIH HHS/United States
- U01 AI041089/AI/NIAID NIH HHS/United States
- U01 HD041983/HD/NICHD NIH HHS/United States
- HL079533/HL/NHLBI NIH HHS/United States
- HL72705/HL/NHLBI NIH HHS/United States
- R01 HL072705/HL/NHLBI NIH HHS/United States
- N01 HR096043/HR/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
