

Alberta Stroke Program Early CT Scoring of CT perfusion in early stroke visualization and assessment
- PMID: 17921237
- PMCID: PMC8134254
- DOI: 10.3174/ajnr.A0689
Alberta Stroke Program Early CT Scoring of CT perfusion in early stroke visualization and assessment
Abstract
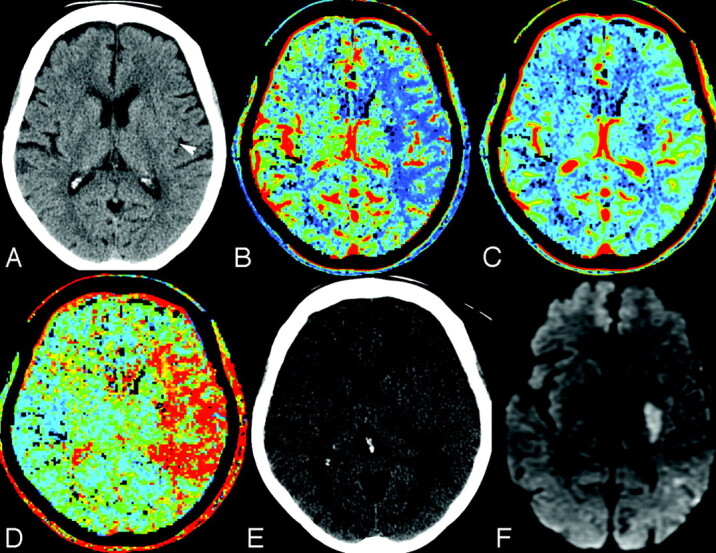
Background and purpose: Qualitative CT perfusion (CTP) assessment by using the Alberta Stroke Program Early CT Score (ASPECTS) allows rapid calculation of infarct extent for middle cerebral artery infarcts. Published thresholds exist for noncontrast CT (NCCT) ASPECTS, which may distinguish outcome/complication risk, but early ischemic signs are difficult to detect. We hypothesized that different ASPECTS thresholds exist for CTP parameters versus NCCT and that these may be superior at predicting clinical and radiologic outcome in the acute setting.
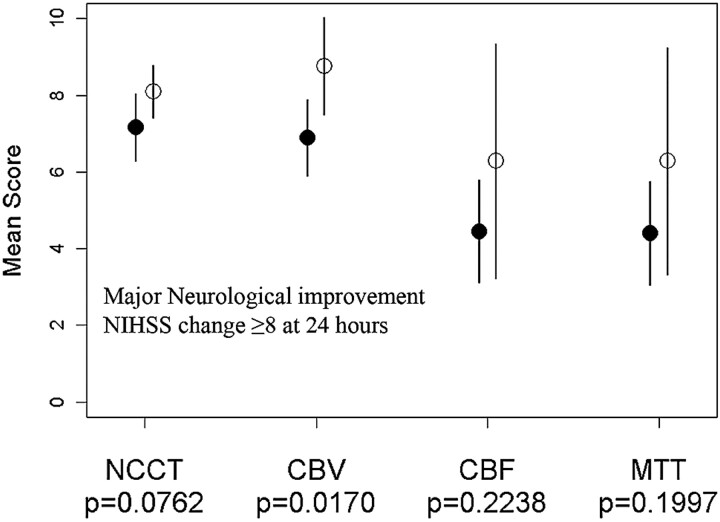
Materials and methods: Thirty-six baseline acute stroke NCCT and CTP studies within 3 hours of symptoms were blindly reviewed by 3 neuroradiologists, and ASPECTS were assigned. Treatment response was defined as major neurologic improvement when a > or =8-point National Institutes of Health Stroke Scale improvement at 24 hours occurred. Follow-up NCCT ASPECTS and 90-day modified Rankin score (mRS) were radiologic and clinical reference standards. Receiver operating characteristic curves derived optimal thresholds for outcome.
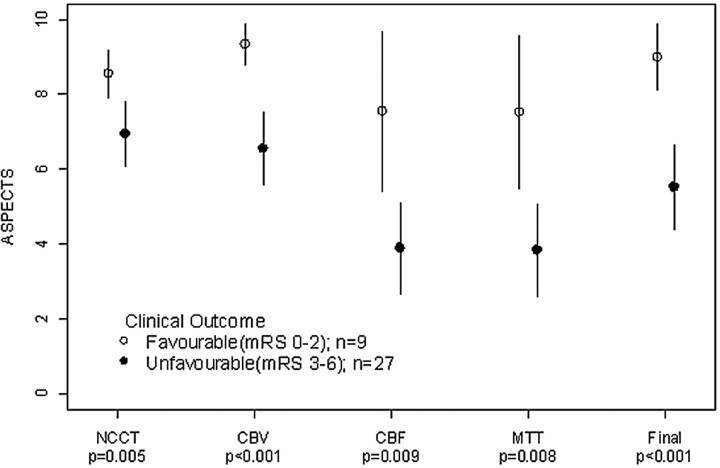
Results: Cerebral blood volume and NCCT ASPECTS had similar radiologic correlations (0.6 and 0.5, respectively) and best predicted infarct size in the absence of major neurologic improvement. A NCCT ASPECT threshold of 7 and a cerebral blood volume threshold of 8 discriminated patients with poor follow-up scans (P < .0002 and P = .0001) and mRS < or =2 (P = .001 and P < .001). Only cerebral blood volume predicted major neurologic improvement (P = .02). Interobserver agreement was substantial (intraclass correlation coefficient, 0.69). Cerebral blood volume ASPECTS sensitivity, specificity, positive predictive value, and negative predictive value for clinical outcome were 60%, 100%, 100%, and 45%, respectively. No patients with cerebral blood volume ASPECTS <8 achieved good clinical outcome.
Conclusion: Cerebral blood volume ASPECTS is equivalent to NCCT for predicting radiologic outcome but may have an additional benefit in predicting patients with major neurologic improvement.
Figures
References
-
- von Kummer R, Nolte PN, Schnittger H, et al. Detectability of cerebral hemisphere ischaemic infarcts by CT within 6 h of stroke. Neuroradiology 1996;38:31–33 - PubMed
-
- Mullins ME, Lev MH, Schellingerhout D, et al. Influence of availability of clinical history on detection of early stroke using unenhanced CT and diffusion-weighted MR imaging. AJR Am J Roentgenol 2002;179:223–28 - PubMed
-
- Lev MH, Farkas J, Gemmete JJ, et al. Acute stroke: improved nonenhanced CT detection–benefits of soft-copy interpretation by using variable window width and center level settings. Radiology 1999;213:150–55 - PubMed
-
- Barber PA, Demchuk AM, Zhang J, et al. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy: ASPECTS Study Group—Alberta Stroke Programme Early CT Score. Lancet 2000;355:1670–74 - PubMed
-
- Coutts SB, Lev MH, Eliasziw M, et al. ASPECTS on CTA source images versus unenhanced CT: added value in predicting final infarct extent and clinical outcome. Stroke 2004;35:2472–76 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical