

A novel subset of putative stem/progenitor CD34+Oct-4+ cells is the major target for SARS coronavirus in human lung
- PMID: 17923501
- PMCID: PMC2118498
- DOI: 10.1084/jem.20070462
A novel subset of putative stem/progenitor CD34+Oct-4+ cells is the major target for SARS coronavirus in human lung
Abstract
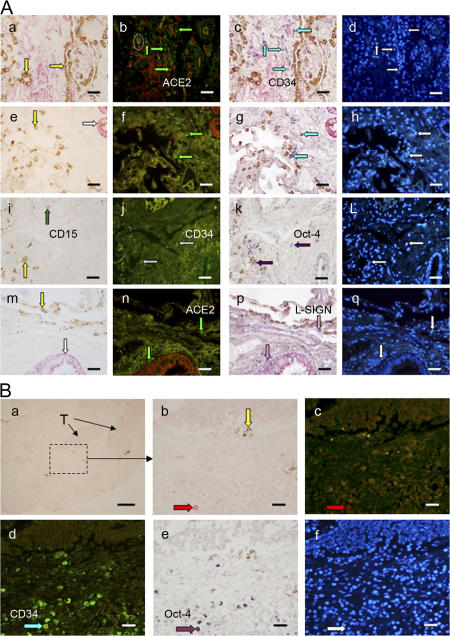
Identification of the nature of severe acute respiratory syndrome (SARS)-infected cells is crucial toward understanding the pathogenesis. Using multicolor colocalization techniques, we previously reported that SARS(+) cells in the lung of fatally infected patients expressed the only known functional receptor, angiotensin-converting enzyme 2, and also a binding receptor, liver/lymph node-specific ICAM-3-grabbing non-integrin (CD209L). In this study, we show that SARS-infected cells also express the stem/progenitor cell markers CD34 and Oct-4, and do not express cytokeratin or surfactant. These putative lung stem/progenitor cells can also be identified in some non-SARS individuals and can be infected by SARS-coronavirus ex vivo. Infection of these cells may contribute to the loss of lung repair capacity that leads to respiratory failure as clinically observed.
Figures


References
-
- Ksiazek, T.G., D. Erdman, C.S. Goldsmith, S.R. Zaki, T. Peret, S. Emery, S. Tong, C. Urbani, J.A. Comer, W. Lim, et al. 2003. A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 348:1953–1966. - PubMed
-
- Drosten, C., S. Gunther, W. Preiser, S. van der Werf, H.R. Brodt, S. Becker, H. Rabenau, M. Panning, L. Kolesnikova, R.A. Fouchier, et al. 2003. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N. Engl. J. Med. 348:1967–1976. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
