

Preoperative warming combined with intraoperative skin-surface warming does not avoid hypothermia caused by spinal anesthesia in patients with midazolam premedication
- PMID: 17923938
- PMCID: PMC11020579
- DOI: 10.1590/s1516-31802007000300004
Preoperative warming combined with intraoperative skin-surface warming does not avoid hypothermia caused by spinal anesthesia in patients with midazolam premedication
Abstract
Context and objective: Inadvertent perioperative hypothermia is common during spinal anesthesia and after midazolam administration. The aim of this study was to evaluate the effects of intraoperative skin-surface warming with and without 45 minutes of preoperative warming in preventing intraoperative and postoperative hypothermia caused by spinal anesthesia in patients with midazolam premedication.
Design and setting: Prospective and randomized study at Hospital das Clínicas, Universidade Estadual Paulista, Botucatu.
Methods: Thirty patients presenting American Society of Anesthesiologists (ASA) physical status I and II who were scheduled for elective lower abdominal surgery were utilized. The patients received midazolam premedication (7.5 mg by intramuscular injection) and standard spinal anesthesia. Ten patients (Gcontrol) received preoperative and intraoperative passive thermal insulation. Ten patients (Gpre+intra) underwent preoperative and intraoperative active warming. Ten patients (Gintra) were only warmed intraoperatively.
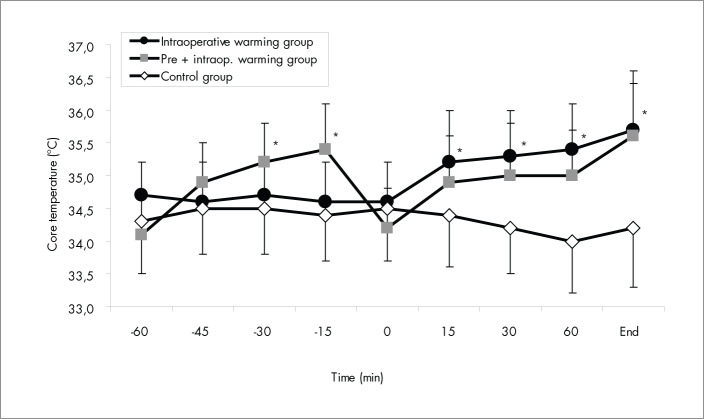
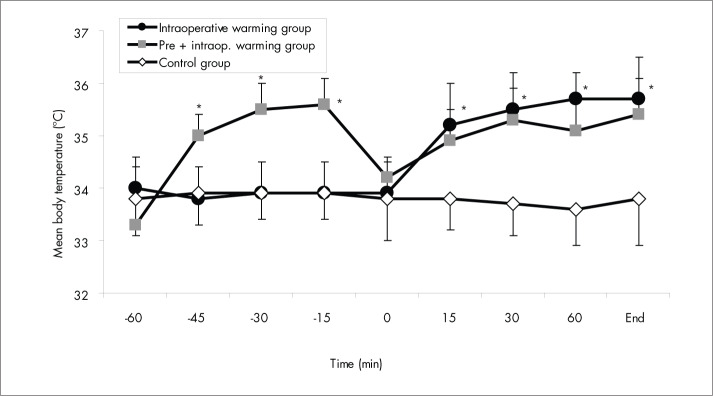
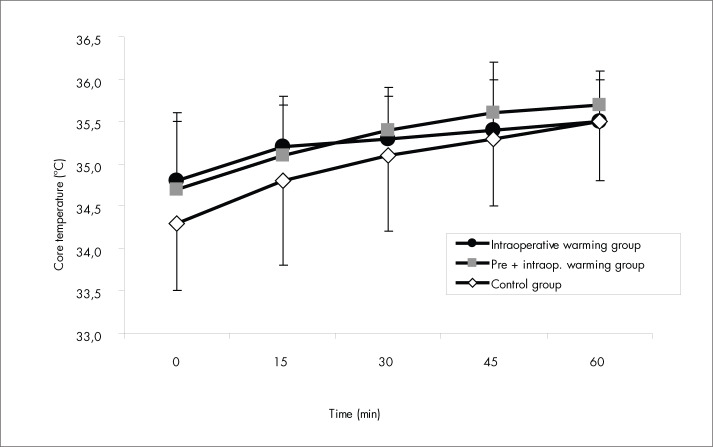
Results: After 45 min of preoperative warming, the patients in Gpre+intra had significantly higher core temperatures than did the patients in the unwarmed groups (Gcontrol and Gintra) before the anesthesia (p < 0.05) but not at the beginning of surgery (p > 0.05). The patients who were warmed intraoperatively had significantly higher core temperatures than did the patients in Gcontrol at the end of surgery (p < 0.05). All the patients were hypothermic at admission to the recovery room (T CORE < 36 degrees C).
Conclusions: Forty-five minutes of preoperative warming combined with intraoperative skin-surface warming does not avoid but minimizes hypothermia caused by spinal anesthesia in patients with midazolam premedication.
CONTEXTO E OBJETIVO:: Hipotermia inadvertida no perioperatório é freqüente durante anestesia subaracnóidea e após a administração de midazolam. O objetivo foi avaliar os efeitos do aquecimento da pele no intra-operatório, associado ou não ao aquecimento da pele durante o período de 45 minutos no pré-operatório, na prevenção de hipotermia intra- e pós-operatória determinada pela anestesia subaracnóidea em pacientes com medicação pré-anestésica com midazolam.
TIPO DE ETUDO E LOCAL:: Estudo prospectivo e aleatório, realizado no Hospital das Clínicas, Universidade Estadual Paulista (Unesp), Botucatu, SP.
MÉTODOS:: O estudo foi realizado em 30 pacientes com estado físico ASA (da Sociedade Norte-americana de Anestesiologistas) I e II submetidos à cirurgia eletiva do abdômen. Como medicação pré-anestésica, utilizou-se o midazolam, 7,5 mg via intramuscular (IM) e anestesia subaracnóidea padrão. Em 10 pacientes (Gcontrole) utilizou-se isolamento térmico passivo; 10 pacientes (Gpré+intra) foram submetidos a aquecimento ativo no pré- e intra-operatório; e 10 pacientes (Gintra) foram aquecidos ativamente somente no intra-operatório.
RESULTADOS:: Após 45 minutos de aquecimento no pré-operatório, os pacientes do Gpré+intra apresentaram temperatura central mais elevada em relação aos dos grupos não aquecidos antes da anestesia (p < 0,05) mas não no início da cirurgia (p > 0,05). Os pacientes que receberam aquecimento no intra-operatório apresentaram temperatura central mais elevada no final da cirurgia em relação aos de Gcontrole (p < 0,05). Todos os pacientes estavam hipotérmicos na admissão da sala de recuperação pós-anestésica (temperatura central < 36° C).
CONCLUSÕES:: 45 minutos de aquecimento no pré-operatório combinado com aquecimento no intra-operatório não evita, mas minimiza a ocorrência de hipotermia determinada pela anestesia subaracnóidea em pacientes que receberam midazolam como medicação pré-anestésica.
Conflict of interest statement
Figures

Similar articles
-
Preoperative combined with intraoperative skin-surface warming avoids hypothermia caused by general anesthesia and surgery.J Clin Anesth. 2003 Mar;15(2):119-25. doi: 10.1016/s0952-8180(02)00512-3. J Clin Anesth. 2003. PMID: 12719051 Clinical Trial.
-
Active perioperative patient warming using a self-warming blanket (BARRIER EasyWarm) is superior to passive thermal insulation: a multinational, multicenter, randomized trial.J Clin Anesth. 2016 Nov;34:547-54. doi: 10.1016/j.jclinane.2016.06.030. Epub 2016 Jul 17. J Clin Anesth. 2016. PMID: 27687449 Clinical Trial.
-
Pre-warming following premedication limits hypothermia before and during anesthesia in Sprague-Dawley rats (Rattus norvegicus).Can J Vet Res. 2021 Apr;85(2):106-111. Can J Vet Res. 2021. PMID: 33883817 Free PMC article.
-
Effects of combined warmed preoperative forced-air and warmed perioperative intravenous fluids on maternal temperature during cesarean section: a prospective, randomized, controlled clinical trial.BMC Anesthesiol. 2020 Feb 26;20(1):48. doi: 10.1186/s12871-020-00970-7. BMC Anesthesiol. 2020. PMID: 32101145 Free PMC article. Clinical Trial.
-
[Non-therapeutic intraoperative hypothermia: prevention and treatment (part II)].Rev Esp Anestesiol Reanim. 2003 Apr;50(4):197-208. Rev Esp Anestesiol Reanim. 2003. PMID: 12825309 Review. Spanish.
Cited by
-
Active body surface warming systems for preventing complications caused by inadvertent perioperative hypothermia in adults.Cochrane Database Syst Rev. 2016 Apr 21;4(4):CD009016. doi: 10.1002/14651858.CD009016.pub2. Cochrane Database Syst Rev. 2016. PMID: 27098439 Free PMC article.
-
Effect of an Insulation Device in Preventing Hypothermia during Magnetic Resonance Imaging Examinations for Dogs and Cats under General Anesthesia.Animals (Basel). 2021 Aug 12;11(8):2378. doi: 10.3390/ani11082378. Animals (Basel). 2021. PMID: 34438834 Free PMC article.
-
Effectiveness of active and passive warming for the prevention of inadvertent hypothermia in patients receiving neuraxial anesthesia: A systematic review and meta-analysis of randomized controlled trials.J Clin Anesth. 2017 May;38:93-104. doi: 10.1016/j.jclinane.2017.01.005. Epub 2017 Jan 31. J Clin Anesth. 2017. PMID: 28372696 Free PMC article.
-
[Risk factors for postoperative hypothermia in the post-anesthetic care unit: a prospective prognostic pilot study].Braz J Anesthesiol. 2019 Mar-Apr;69(2):122-130. doi: 10.1016/j.bjan.2018.10.001. Epub 2019 Jan 23. Braz J Anesthesiol. 2019. PMID: 30685072 Free PMC article.
-
Investigation of inadvertent hypothermia incidence and risk factors.Turk J Surg. 2018 Dec 1;34(4):300-305. doi: 10.5152/turkjsurg.2018.3992. Turk J Surg. 2018. PMID: 30664429 Free PMC article.
References
-
- Szmuk P, Ezri T, Sessler DI, Stein A, Geva D. Spinal anesthesia speeds active postoperative rewarming. Anesthesiology. 1997;87(5):1050–1054. - PubMed
-
- Frank SM, Beattie C, Christopherson R, et al. Epidural versus general anesthesia, ambient operating room temperature, and patient age as predictors of inadvertent hypothermia. Anesthesiology. 1992;77(2):252–257. - PubMed
-
- Frank SM, Shir Y, Raja SN, Fleisher LA, Beattie C. Core hypothermia and skin-surface temperature gradients. Epidural versus general anesthesia and the effects of age. Anesthesiology. 1994;80(3):502–508. - PubMed
-
- Matsukawa T, Sessler DI, Christensen R, Ozaki M, Schroeder M. Heat flow and distribution during epidural anesthesia. Anesthesiology. 1995;83(5):961–967. - PubMed
-
- Ozaki M, Kurz A, Sessler DI, et al. Thermoregulatory thresholds during epidural and spinal anesthesia. Anesthesiology. 1994;81(2):282–288. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
