

An exploratory study with an adaptive continuous intravenous furosemide regimen in neonates treated with extracorporeal membrane oxygenation
- PMID: 17925044
- PMCID: PMC2556764
- DOI: 10.1186/cc6146
An exploratory study with an adaptive continuous intravenous furosemide regimen in neonates treated with extracorporeal membrane oxygenation
Abstract
Introduction: The objective of the present study was to explore a continuous intravenous furosemide regimen that adapts to urine output in neonates treated with extracorporeal membrane oxygenation (ECMO).
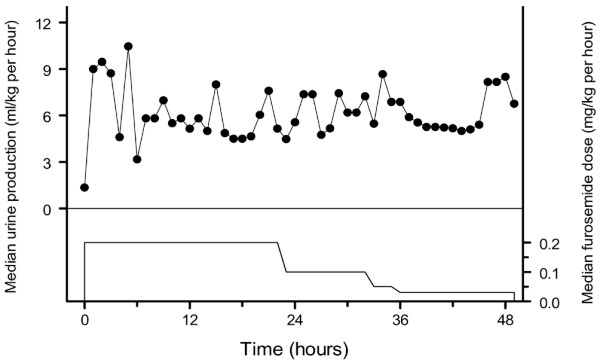
Methods: Seven neonates admitted to a paediatric surgical intensive care unit for ECMO therapy were treated with a furosemide regimen consisting of a loading bolus (1-2 mg/kg) followed by a continuous infusion at 0.2 mg/kg per hour, which was adjusted according to the target urine production of 6 ml/kg per hour. Therapeutic drug monitoring for furosemide concentrations in blood was performed.
Results: The mean +/- standard deviation furosemide dose was 0.17 +/- 0.06 mg/kg per hour, 0.08 +/- 0.04 mg/kg per hour and 0.12 +/- 0.07 mg/kg per hour, respectively, on the first day, second day and third day of the study. The median (range of the urine production of the study subjects) urine production over the consecutive study days was 6.8 (0.8-8.4) mg/kg per hour, 6.0 (4.7-8.9) mg/kg per hour and 5.4 (3.4-10.1) ml/kg per hour. The target urine production was reached after a median time of 7 (3-37) hours. The regimen was haemodynamically well tolerated and the median furosemide serum concentration was 3.1 (0.4-12.9) mug/ml, well below the toxic level.
Conclusion: The evaluated furosemide infusion appears an effective means to reduce volume overload in neonates treated with ECMO. The data of this preliminary study suggest that the starting dose of furosemide was too high, however, because the urine output was excessive and required frequent adaptations. The results of this study therefore indicate that a novel pharmacokinetic/pharmacodynamic model needs to be developed for neonates treated with ECMO.
Figures
Similar articles
-
Evaluation of furosemide regimens in neonates treated with extracorporeal membrane oxygenation.Crit Care. 2006;10(6):R168. doi: 10.1186/cc5115. Crit Care. 2006. PMID: 17140428 Free PMC article.
-
Continuous intravenous furosemide in haemodynamically unstable children after cardiac surgery.Intensive Care Med. 2001 Apr;27(4):711-5. doi: 10.1007/s001340000819. Intensive Care Med. 2001. PMID: 11398698 Clinical Trial.
-
Absence of tolerance and toxicity to high-dose continuous intravenous furosemide in haemodynamically unstable infants after cardiac surgery.Br J Clin Pharmacol. 2007 Dec;64(6):796-803. doi: 10.1111/j.1365-2125.2007.02913.x. Epub 2007 Apr 18. Br J Clin Pharmacol. 2007. PMID: 17441933 Free PMC article.
-
Clinical pharmacology of the loop diuretics furosemide and bumetanide in neonates and infants.Paediatr Drugs. 2012 Aug 1;14(4):233-46. doi: 10.2165/11596620-000000000-00000. Paediatr Drugs. 2012. PMID: 22702741 Review.
-
[Optimal way of administration of high dose intravenous furosemide - continuous infusion or bolus?].Vnitr Lek. 2014 Oct;60(10):885-92. Vnitr Lek. 2014. PMID: 25382011 Review. Czech.
Cited by
-
Optimising drug dosing in patients receiving extracorporeal membrane oxygenation.J Thorac Dis. 2018 Mar;10(Suppl 5):S629-S641. doi: 10.21037/jtd.2017.09.154. J Thorac Dis. 2018. PMID: 29732181 Free PMC article. Review.
-
Acute kidney injury is a frequent complication in critically ill neonates receiving extracorporeal membrane oxygenation: a 14-year cohort study.Crit Care. 2013 Jul 24;17(4):R151. doi: 10.1186/cc12830. Crit Care. 2013. PMID: 23883698 Free PMC article.
-
Pediatric cardiovascular drug dosing in critically ill children and extracorporeal membrane oxygenation.J Cardiovasc Pharmacol. 2011 Aug;58(2):126-32. doi: 10.1097/FJC.0b013e318213aac2. J Cardiovasc Pharmacol. 2011. PMID: 21346597 Free PMC article. Review.
-
Ethacrynic Acid continuous infusions in critically ill pediatric patients.J Pediatr Pharmacol Ther. 2014 Jan;19(1):49-55. doi: 10.5863/1551-6776-19.1.49. J Pediatr Pharmacol Ther. 2014. PMID: 24782692 Free PMC article.
-
Clinical pharmacology of furosemide in neonates: a review.Pharmaceuticals (Basel). 2013 Sep 5;6(9):1094-129. doi: 10.3390/ph6091094. Pharmaceuticals (Basel). 2013. PMID: 24276421 Free PMC article.
References
-
- Journois D. Hemofiltration during cardiopulmonary bypass. Kidney Int Suppl. 1998;66:S174–S177. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
