

Primaquine clears submicroscopic Plasmodium falciparum gametocytes that persist after treatment with sulphadoxine-pyrimethamine and artesunate
- PMID: 17925871
- PMCID: PMC1995753
- DOI: 10.1371/journal.pone.0001023
Primaquine clears submicroscopic Plasmodium falciparum gametocytes that persist after treatment with sulphadoxine-pyrimethamine and artesunate
Abstract
Background: P. falciparum gametocytes may persist after treatment with sulphadoxine-pyrimethamine (SP) plus artesunate (AS) and contribute considerably to malaria transmission. We determined the efficacy of SP+AS plus a single dose of primaquine (PQ, 0.75 mg/kg) on clearing gametocytaemia measured by molecular methods.
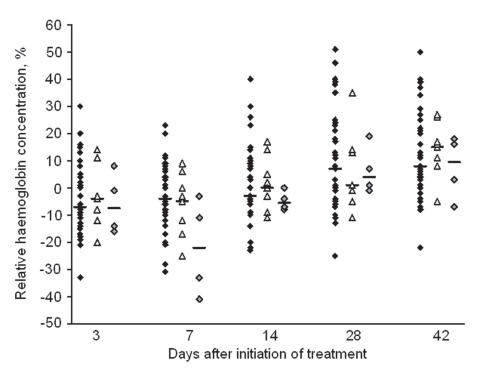
Methodology: The study was conducted in Mnyuzi, an area of hyperendemic malaria in north-eastern Tanzania. Children aged 3-15 years with uncomplicated P. falciparum malaria with an asexual parasite density between 500-100,000 parasites/microL were randomized to receive treatment with either SP+AS or SP+AS+PQ. P. falciparum gametocyte prevalence and density during the 42-day follow-up period were determined by real-time nucleic acid sequence-based amplification (QT-NASBA). Haemoglobin levels (Hb) were determined to address concerns about haemolysis in G6PD-deficient individuals.
Results: 108 individuals were randomized. Pfs25 QT-NASBA gametocyte prevalence was 88-91% at enrolment and decreased afterwards for both treatment arms. Gametocyte prevalence and density were significantly lower in children treated with SP+AS+PQ. On day 14 after treatment 3.9% (2/51) of the SP+AS+PQ treated children harboured gametocytes compared to 62.7% (32/51) of those treated with SP+AS (p<0.001). Hb levels were reduced in the week following treatment with SP+AS+PQ and this reduction was related to G6PD deficiency. The Hb levels of all patients recovered to pre-treatment levels or greater within one month after treatment.
Conclusions: PQ clears submicroscopic gametocytes after treatment with SP+AS and the persisting gametocytes circulated at densities that are unlikely to contribute to malaria transmission. For individuals without severe anaemia, addition of a single dose of PQ to an efficacious antimalarial drug combination is a safe approach to reduce malaria transmission following treatment.
Trial registration: Controlled-Trials.com ISRCTN61534963.
Conflict of interest statement
Figures



References
-
- World Health Organization. Guidelines for the treatment of malaria. WHO/HTM/MAL/2006. 2006;1108
-
- von Seidlein L, Greenwood BM. Mass administrations of antimalarial drugs. Trends Parasitol. 2003;19:452–460. - PubMed
-
- Adjuik M, Babiker A, Garner P, Olliaro P, Taylor W, White N. Artesunate combinations for treatment of malaria: meta-analysis. Lancet. 2004;363:9–17. - PubMed
-
- Bousema JT, Schneider P, Gouagna LC, Drakeley CJ, Tostmann A, et al. Moderate Effect of Artemisinin-Based Combination Therapy on Transmission of Plasmodium falciparum. J Infect Dis. 2006;193:1151–1159. - PubMed
-
- Drakeley CJ, Jawara M, Targett GAT, Walraven G, Obisike U, et al. Addition of artesunate to chloroquine for treatment of Plasmodium falciparum malaria in Gambian children causes a significant but short-lived reduction in infectiousness for mosquitoes. Trop Med Int Health. 2004;9:53–61. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
