

Coinfection of Japanese encephalitis with neurocysticercosis: an imaging study
- PMID: 17928378
- PMCID: PMC8119090
- DOI: 10.3174/ajnr.A0769
Coinfection of Japanese encephalitis with neurocysticercosis: an imaging study
Abstract
Background and purpose: Coinfection of neurocysticercosis (NCC) and Japanese encephalitis (JE) has been advocated as more than a chance occurrence resulting in poor outcome. We undertook this study to determine whether the association of the 2 infections is more than a chance occurrence, to define the imaging characteristics of coinfections, and to explore the synergistic effect of NCC in JE.
Materials and methods: Sixty-two patients with JE were studied by MR imaging and CT. CT was done in 53 and MR imaging in 53 patients. The diagnosis of JE was established by CSF JE virus immunoglobulin M capture (MAC) enzyme-linked immunosorbent assay (ELISA). NCC was diagnosed from imaging. A control group of 385 patients was evaluated by imaging for prevalence of NCC in the general population.
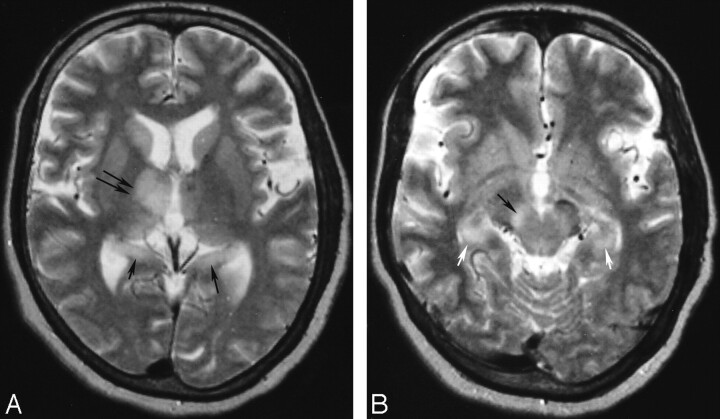
Results: A significantly high association of NCC with JE (19.3%) was observed in comparison with prevalence of NCC in control subjects (1.04%; P = .0003). JE lesions in coinfection were significantly asymmetric with lateralization to the side of the brain having the maximum NCC or a cyst with edema. The JE lesions in coinfections were more florid, with a significantly higher proportion of abnormal CT scans and more abnormal MR imaging. Coinfections were significantly more common in children. Significantly lower CSF MAC-ELISA units in patients with coinfection reflected low CSF IgM levels, suggesting altered immune status.
Conclusion: In our series, there was a strong association between JE and NCC, and, thus, this coinfection was more than a chance occurrence.
Figures



References
-
- Kabilan L, Rajendran R, Arunachalam N, et al. Japanese encephalitis in India: an overview. Indian J Paediatr 2004;71:609–15 - PubMed
-
- Kalita J, Misra UK. Comparision of CT scan and MRI findings in the diagnosis of Japanese encephalitis. J Neurol Sci 2000;174:3–8 - PubMed
-
- Shoji H, Kida H, Hino H, et al. Magnetic resonance imaging findings in Japanese encephalitis. White matter lesions. J Neuroimaging 1994;4:206–11 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical