

Diagnostic accuracy of CT angiography with matched mask bone elimination for detection of intracranial aneurysms: comparison with digital subtraction angiography and 3D rotational angiography
- PMID: 17928381
- PMCID: PMC8119108
- DOI: 10.3174/ajnr.A0741
Diagnostic accuracy of CT angiography with matched mask bone elimination for detection of intracranial aneurysms: comparison with digital subtraction angiography and 3D rotational angiography
Abstract
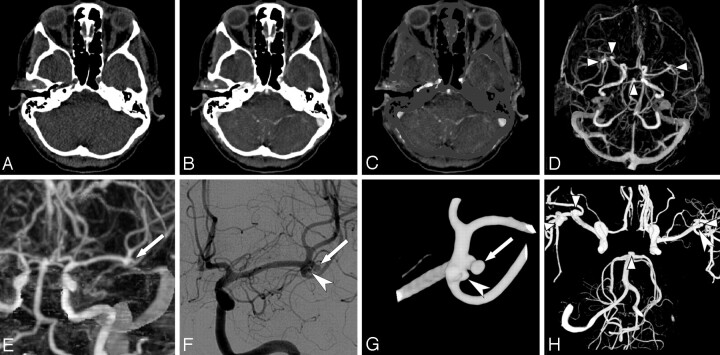
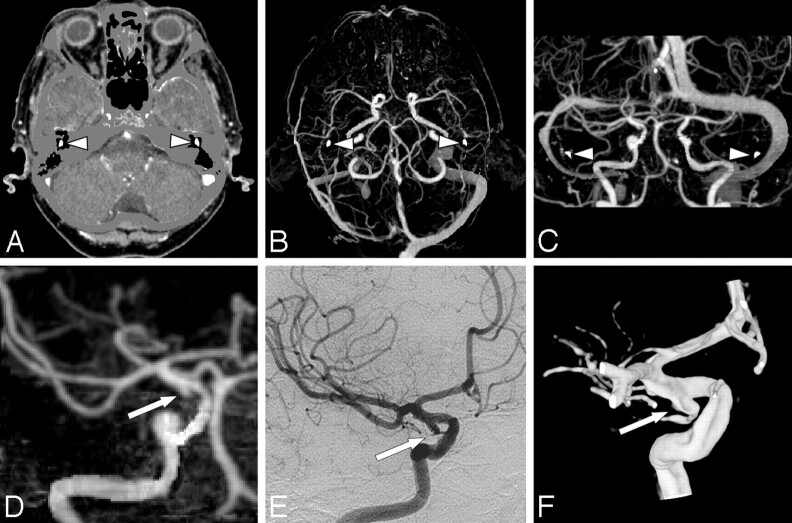
Background and purpose: Our aim was to determine the diagnostic accuracy of multisection CT angiography combined with matched mask bone elimination (CTA-MMBE) for detection of intracranial aneurysms compared with digital subtraction angiography (DSA) and 3D rotational angiography (3DRA).
Materials and methods: Between January 2004 and February 2006, 108 patients who presented with clinically suspected subarachnoid hemorrhage underwent both CTA-MMBE and DSA for diagnosis of an intracranial aneurysm. Two neuroradiologists, independently, evaluated 27 predefined vessel locations in the CTA-MMBE images for the presence of an aneurysm. After consensus, diagnostic accuracy of CTA was calculated per predefined location and per patient. Interobserver agreement was calculated with kappa statistics.
Results: In 88 patients (81%), 117 aneurysms (82 ruptured, 35 unruptured) were present on DSA. CTA-MMBE detected all ruptured aneurysms except 1. Overall specificity, sensitivity, positive predictive value, and negative predictive value of CTA-MMBE were 0.99, 0.90, 0.98, and 0.95 per patient and 0.91, 1.00, 0.97, and 0.99 per location, respectively. Sensitivity was 0.99 for aneurysms >/=3 mm and 0.38 for aneurysms <3 mm. Interobserver agreement for aneurysm detection was excellent (kappa value of 0.92 per location and 0.80 per patient).
Conclusion: CTA-MMBE is accurate in detecting intracranial aneurysms in any projection without overprojecting bone. CTA-MMBE has limited sensitivity in detecting very small aneurysms. Our data suggest that DSA and 3DRA can be limited to the vessel harboring the ruptured aneurysm before endovascular treatment, after detection of a ruptured aneurysm with CTA.
Figures
Similar articles
-
Dual-energy CT angiography in the evaluation of intracranial aneurysms: image quality, radiation dose, and comparison with 3D rotational digital subtraction angiography.AJR Am J Roentgenol. 2010 Jan;194(1):23-30. doi: 10.2214/AJR.08.2290. AJR Am J Roentgenol. 2010. PMID: 20028901
-
Detection of aneurysms by 64-section multidetector CT angiography in patients acutely suspected of having an intracranial aneurysm and comparison with digital subtraction and 3D rotational angiography.AJNR Am J Neuroradiol. 2008 Mar;29(3):594-602. doi: 10.3174/ajnr.A0848. Epub 2007 Dec 7. AJNR Am J Neuroradiol. 2008. PMID: 18065510 Free PMC article.
-
Digital subtraction CT angiography for detection of intracranial aneurysms: comparison with three-dimensional digital subtraction angiography.Radiology. 2012 Feb;262(2):605-12. doi: 10.1148/radiol.11110486. Epub 2011 Dec 5. Radiology. 2012. PMID: 22143927
-
Comprehensive review of imaging of intracranial aneurysms and angiographically negative subarachnoid hemorrhage.Neurosurg Focus. 2019 Dec 1;47(6):E20. doi: 10.3171/2019.9.FOCUS19653. Neurosurg Focus. 2019. PMID: 31786554 Review.
-
Subarachnoid Hemorrhage with Negative Initial Digital Subtraction Angiography: Subsequent Detection of Aneurysms and Complication Rates of Repeated Angiography.J Neurol Surg A Cent Eur Neurosurg. 2023 Mar;84(2):167-173. doi: 10.1055/s-0042-1748771. Epub 2022 Oct 27. J Neurol Surg A Cent Eur Neurosurg. 2023. PMID: 36302519 Review.
Cited by
-
Comparison of bone subtraction CT angiography with standard CT angiography for evaluating circle of Willis in normal dogs.J Vet Sci. 2023 Sep;24(5):e65. doi: 10.4142/jvs.23121. J Vet Sci. 2023. PMID: 38031644 Free PMC article.
-
Clinical practice guideline for the management of intracranial aneurysms.Neurointervention. 2014 Sep;9(2):63-71. doi: 10.5469/neuroint.2014.9.2.63. Epub 2014 Sep 3. Neurointervention. 2014. PMID: 25426300 Free PMC article. Review.
-
Simulation study of Hemodynamic in Bifurcations for Cerebral Arteriovenous Malformation using Electrical Analogy.J Biomed Phys Eng. 2017 Jun 1;7(2):143-154. eCollection 2017 Jun. J Biomed Phys Eng. 2017. PMID: 28580336 Free PMC article.
-
Peripheral ophthalmic artery aneurysm.Neurosurg Rev. 2011 Jan;34(1):29-38. doi: 10.1007/s10143-010-0290-5. Epub 2010 Oct 15. Neurosurg Rev. 2011. PMID: 20949300 Review.
-
Subtracted 3D CT angiography for the evaluation of intracranial aneurysms in 256-slice multidetector CT: usefulness of the 80-kVp plus compact contrast medium bolus protocol.Eur Radiol. 2013 Nov;23(11):3012-9. doi: 10.1007/s00330-013-2928-5. Epub 2013 Jun 8. Eur Radiol. 2013. PMID: 23749226 Clinical Trial.
References
-
- Kouskouras C, Charitanti A, Giavroglou C, et al. Intracranial aneurysms: evaluation using CTA and MRA—correlation with DSA and intraoperative findings. Neuroradiology 2004;46:842–50 - PubMed
-
- Karamessini MT, Kagadis GC, Petsas T, et al. CT angiography with three-dimensional techniques for the early diagnosis of intracranial aneurysms: comparison with intra-arterial DSA and the surgical findings. Eur J Radiol 2004;49:212–23 - PubMed
-
- Hoh BL, Cheung AC, Rabinov JD, et al. Results of a prospective protocol of computed tomographic angiography in place of catheter angiography as the only diagnostic and pretreatment planning study for cerebral aneurysms by a combined neurovascular team. Neurosurgery 2004;54:1329–40 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical