

The use of individually tailored environmental supports to improve medication adherence and outcomes in schizophrenia
- PMID: 17932089
- PMCID: PMC2632420
- DOI: 10.1093/schbul/sbm111
The use of individually tailored environmental supports to improve medication adherence and outcomes in schizophrenia
Abstract
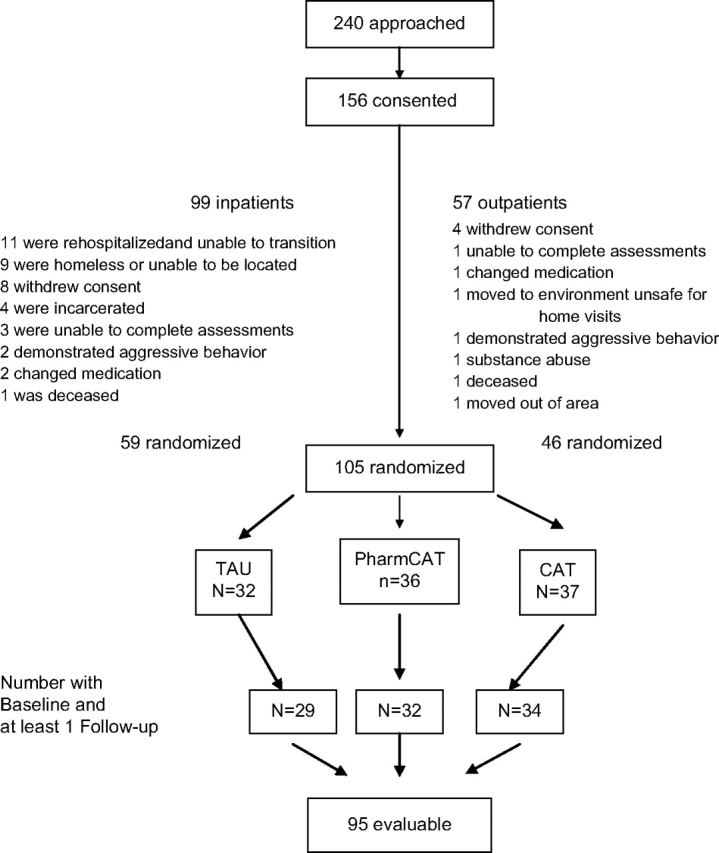
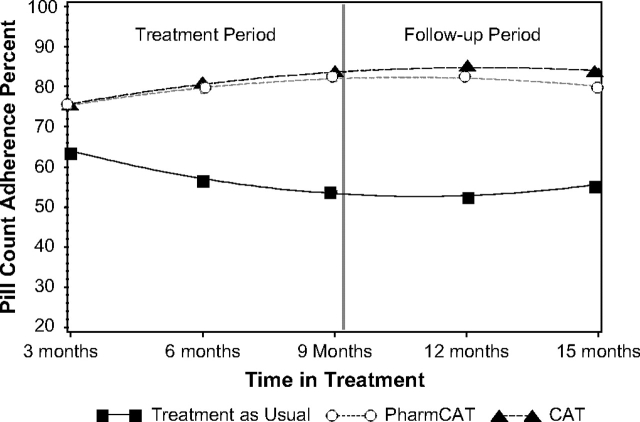
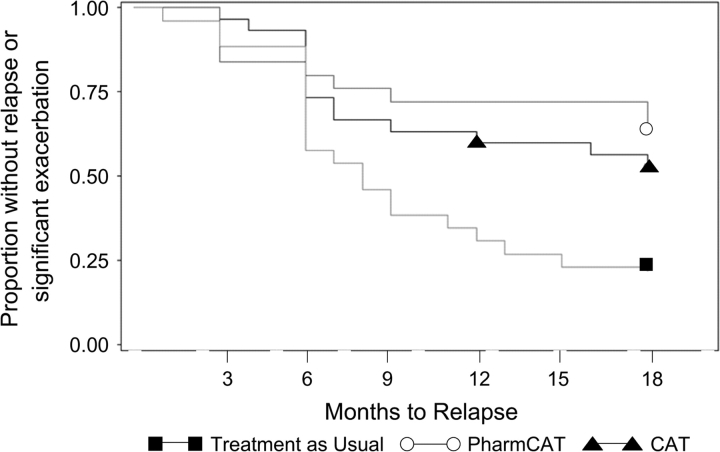
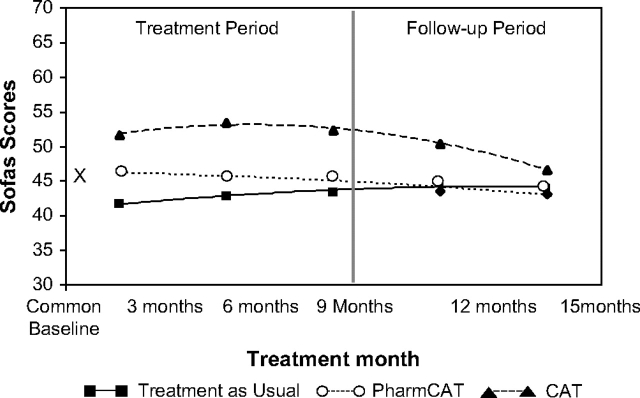
Cognitive adaptation training (CAT) is a psychosocial treatment that uses environmental supports such as signs, checklists, alarms, and the organization of belongings to cue and sequence adaptive behaviors in the home. Ninety-five outpatients with schizophrenia (structured clinical interview for diagnosis, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) were randomly assigned to (1) Full-CAT (CAT focused on many aspects of community adaptation including grooming, care of living quarters, leisure skills, social and role performance, and medication adherence), (2) Pharm-CAT (CAT focused only on medication and appointment adherence), or (3) treatment as usual (TAU). Treatment lasted for 9 months, and patients were followed for 6 months after the withdrawal of home visits. Medication adherence (assessed during unannounced, in-home pill counts) and functional outcomes were assessed at 3-month intervals. Results of mixed-effects regression models indicated that both CAT and Pharm-CAT treatments were superior to TAU for improving adherence to prescribed medication (P < .0001). Effects on medication adherence remained significant when home visits were withdrawn. Full-CAT treatment improved functional outcome relative to Pharm-CAT and TAU (P < .0001). However, differences for functional outcome across groups decreased following the withdrawal of home visits and were no longer statistically significant at the 6-month follow-up. Survival time to relapse or significant exacerbation was significantly longer in both CAT and Pharm-CAT in comparison to TAU (.004). Findings indicate that supports targeting medication adherence can improve and maintain this behavior. Comprehensive supports targeting multiple domains of functioning are necessary to improve functional outcomes. Maintenance of gains in functional outcome may require some form of continued intervention.
Figures
References
-
- Bell MD, Fiszdon J, Bryson G, Wexler BE. Effects of neurocognitive enhancement therapy in schizophrenia: normalisation of memory performance. Cognit Neuropsychiatry. 2004;9:199–211. - PubMed
-
- Velligan DI, Bow-Thomas CC, Huntzinger CD, et al. Randomized controlled trial of the use of compensatory strategies to enhance adaptive functioning in outpatients with schizophrenia. Am J Psychiatry. 2000;157:1317–1323. - PubMed
-
- Wykes T, Reeder C. Cognitive Remediation Therapy for Schizophrenia: An Introduction. New York, NY: Brunner-Routledge; 2005.
-
- Medalia A, Revheim N, Casey M. The remediation of problem-solving skills in schizophrenia. Schizophr Bull. 2001;27:259–267. - PubMed
-
- Medalia A, Revheim N, Casey M. Remediation of memory disorders in schizophrenia. Psychol Med. 2000;30:1451–1459. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
