

Review
doi: 10.1007/s00247-007-0610-2.
Epub 2007 Oct 12.
Malfunctioning central venous catheters in children: a diagnostic approach
Affiliations
- PMID: 17932667
- PMCID: PMC2292495
- DOI: 10.1007/s00247-007-0610-2
Item in Clipboard
Review
Malfunctioning central venous catheters in children: a diagnostic approach
Pediatr Radiol.
2008 Apr.
Abstract
Central venous access is increasingly becoming the domain of the radiologist, both in terms of the insertion of central venous catheters (CVCs) and in the subsequent management of these lines. This article seeks to provide an overview of the CVC types available for paediatric patients and a more detailed explanation of the spectrum of complications that may lead to catheter malfunction. A standard catheter contrast study or 'linogram' technique is described. The normal appearances of such a study and a detailed pictorial review of abnormal catheter studies are provided, together with a brief overview of how information from catheter investigations can guide the management of catheter complications.
Figures

A 4F single-lumen Hickman (Bard Access Systems, Salt Lake City, Utah) catheter for tunnelled central venous access. Inset illustrates the Dacron ingrowth cuff
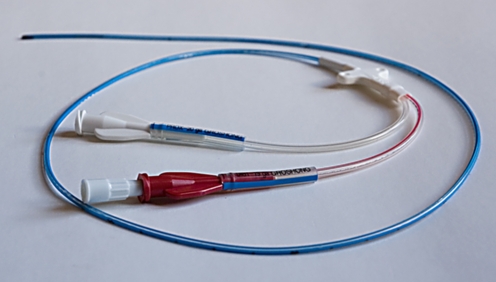
A permanent (tunnelled) haemodialysis catheter with staggered tip for optimal flow rates (12.5F Vas-Cath Soft Cell; Bard Access Systems, Salt Lake City, Utah)

A totally implantable port (Bard Access Systems, Salt Lake City, Utah) with reservoir and 6.6F catheter. Inset illustrates the specialized noncoring port access needle

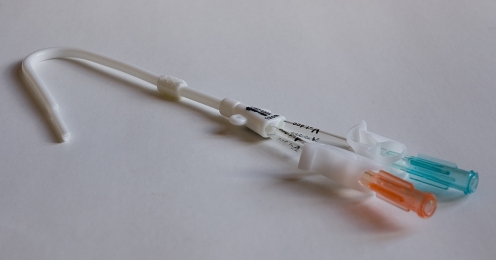
A triple-lumen 7F catheter (Arrow-Howes; Arrow International, Reading, Pa.) for short-term nontunnelled central venous access
A double-lumen 5F PICC (Bard Access Systems, Salt Lake City, Utah)
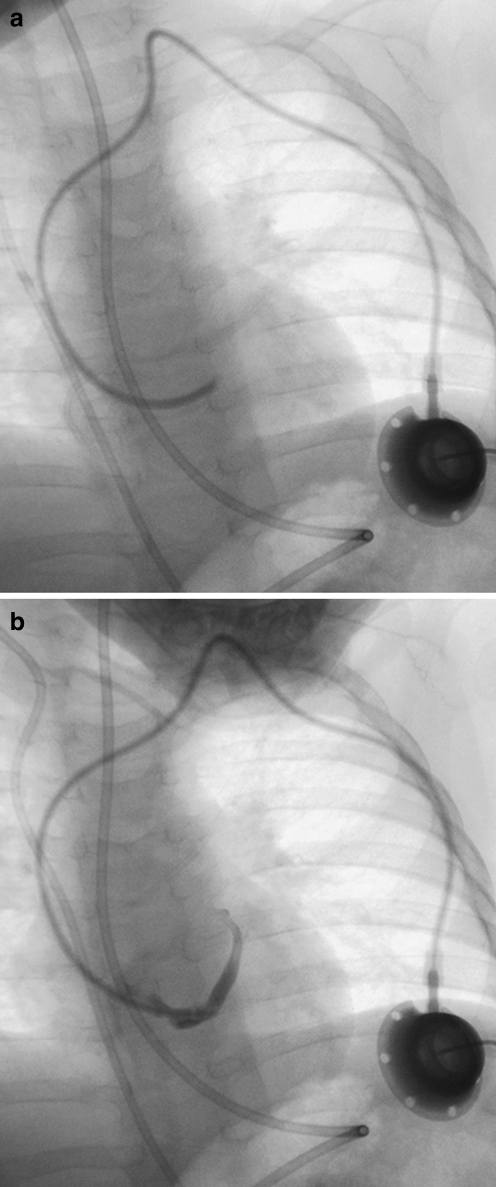
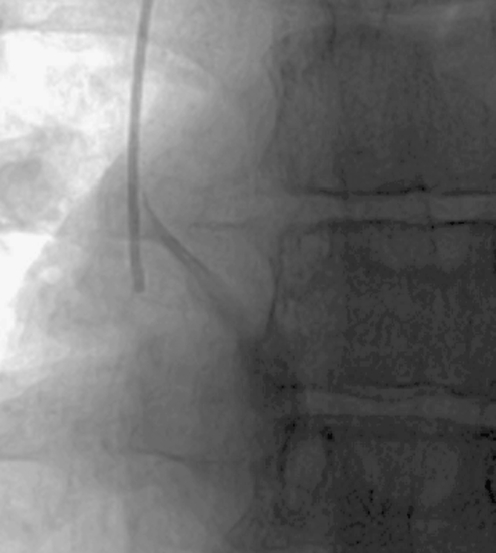
Misplaced catheter. a Fluoroscopic image of a 10-month-old male with a portacath in situ, the tip of which has been placed into the coronary sinus. b The position of the tip is confirmed by a contrast medium study
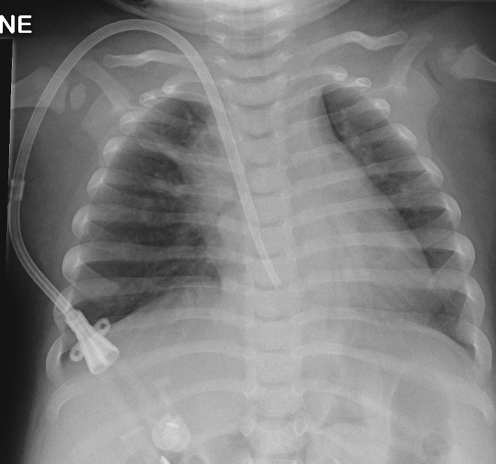
A chest radiograph in a 13-month-old male with a permanent haemodialysis catheter, the tip of which lies at or beyond the level of the tricuspid valve causing intermittently poor flow rates
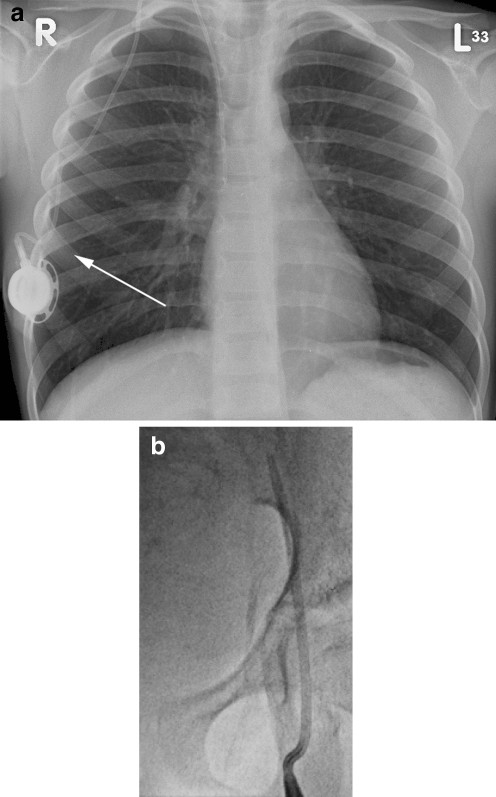
Kinking of the catheter. a Chest radiograph of a 6-year-old male with a portacath in situ. The catheter is kinked just beyond the reservoir (arrow). b Fluoroscopic image of a femoral temporary dialysis catheter in a 15-year-old male. The catheter is kinked at the vessel entry site, causing poor flow rates
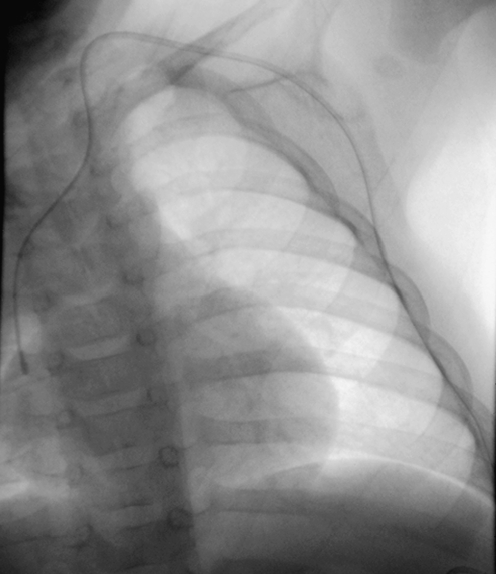
Fluoroscopic image of a tunnelled catheter in a 2-year-old child. The catheter has twisted in the soft tissues of the neck, causing the catheter tip to be partially withdrawn (arrow)
Kinking of the catheter. a, b AP (a) and lateral (b) views of a portacath in a 2-year-old female demonstrating sharp angulation of the proximal catheter, limiting infusion flow rates. The kink is not clearly seen on the AP view
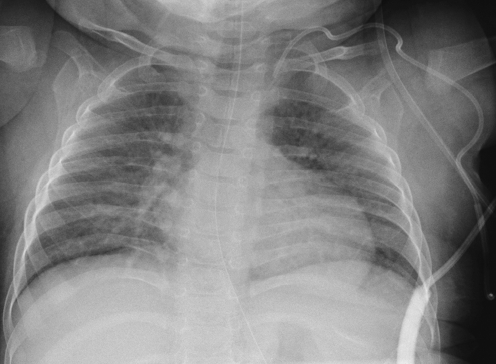
Chest radiograph of a 9-month-old infant with a tunnelled CVC in situ. The catheter has migrated back into the redundant soft tissues of the neck and chest wall
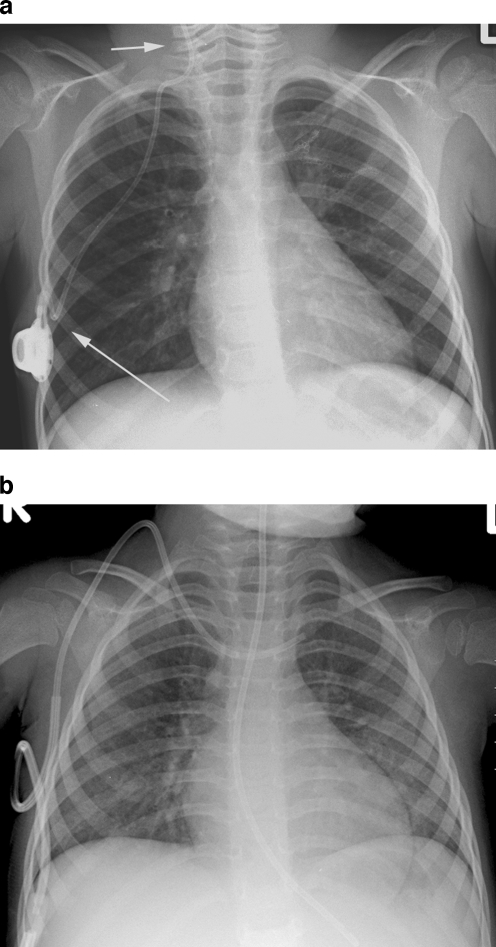
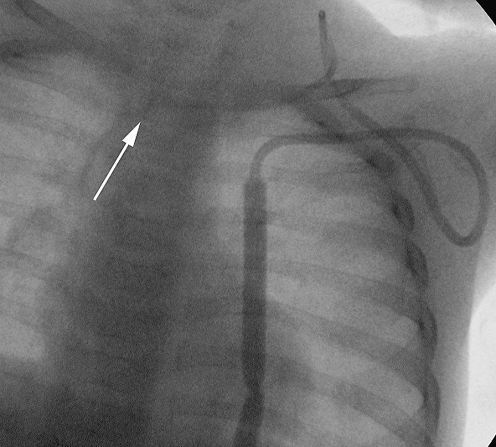
Migration of the catheter tip. a Chest radiograph of a 4-year-old male with a portacath in situ. The catheter tip lies in the right internal jugular vein (short arrow). Note that the proximal catheter is also kinked (long arrow). b Chest radiograph of a 2-year-old female with a tunnelled CVC in situ. The catheter tip lies in the left brachiocephalic vein
Fluoroscopic imaging of a tunnelled catheter in a 4-month-old female. The entire catheter is imaged during slow instillation of contrast medium
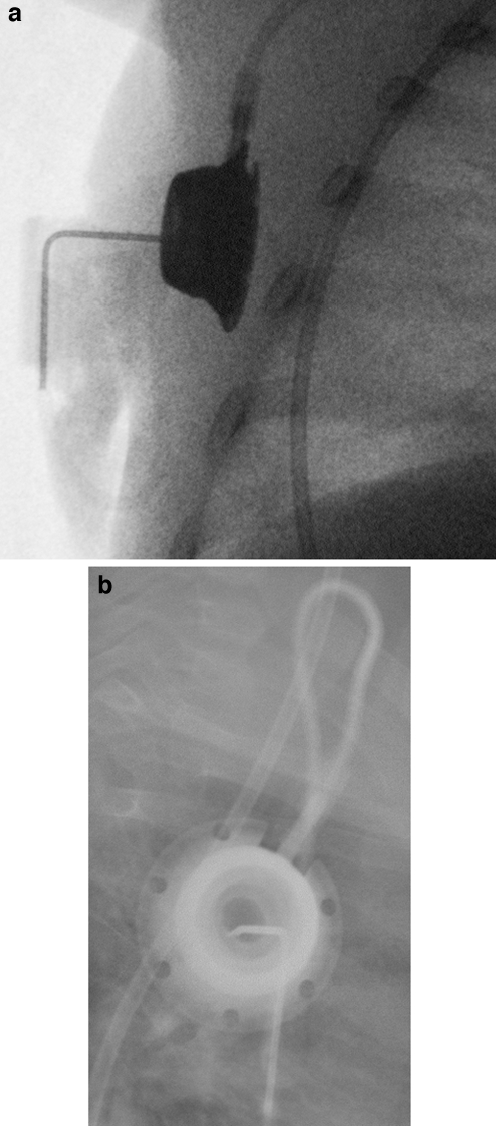
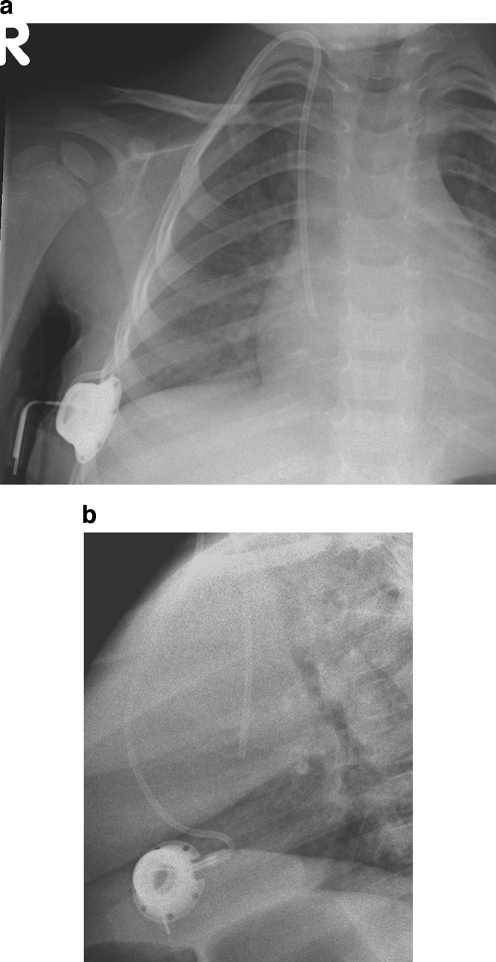
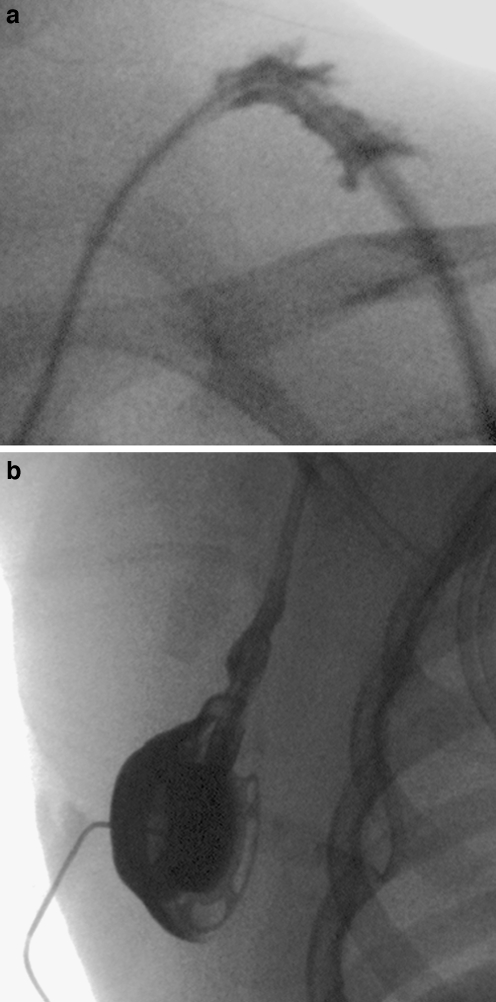
Normal portacath. a, b Tangential (a) and en face (b) views of a portacath reservoir in a 7-year-old male. Note that in both views there is normal opacification of the reservoir during contrast medium instillation
Fluoroscopic image of contrast medium flowing freely from the catheter tip in an 8-year-old male. The contrast medium immediately fans out to fill the right atrium
Normal appearance of the contrast medium jet exiting the side hole of a PICC
Catheter narrowing. a Image acquired during contrast injection through a double-lumen catheter in a 7-year-old male. The catheter is damaged at the site of previous kinks or catheter clamps (arrows). b Focal narrowing of the opacified lumen of a PICC (arrow) in a 3-year-old male where the skin suture device has been attached to the catheter too tightly
Extravasation. a Extravasation of contrast medium into the soft tissues at the site of a catheter break. b Contrast medium is seen leaking from a break in the connection between the portacath reservoir and the catheter
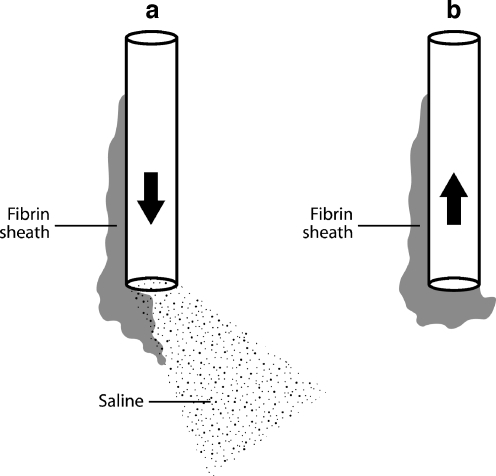
Line drawing demonstrating the effect of a fibrin sheath. a Flushing the catheter displaces the sheath or thrombus from the catheter tip and allows saline to exit the lumen. b Attempted aspiration sucks the sheath back onto the catheter tip, causing withdrawal occlusion

Fluoroscopic contrast study of a haemodialysis catheter in a 9-year-old female. The lumen with a more distal tip has been opacified. The catheter is too long and the distal tip lies up against the inferior wall of the right atrium, causing the contrast jet to be deflected
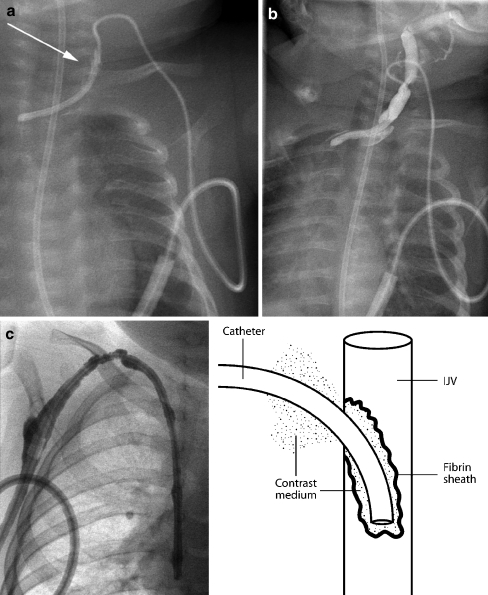
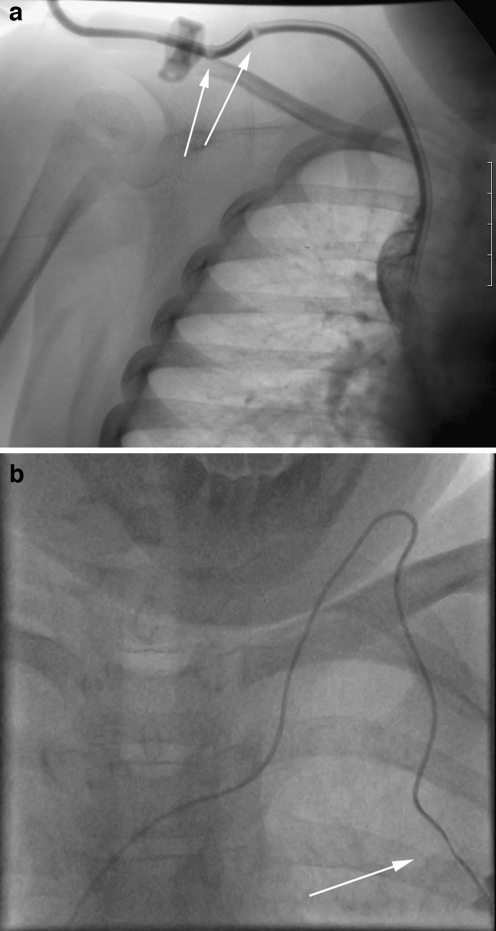
Fibrin sheaths. a, b Contrast medium is instilled into a tunnelled catheter in a 4-month-old child. The catheter has been partially pulled back and the tip lies within the left brachiocephalic vein. A fibrin sheath occludes the catheter. Instead of flowing away from the catheter tip, contrast medium tracks back along the side of the catheter (aarrow) and extravasates into the tissues of the neck (b). c Contrast study performed in a 2-year-old child with a catheter occluded by a fibrin sheath. Contrast medium tracks back along the catheter and into the subcutaneous tunnel, outlining the cuff, as shown diagrammatically in the line drawing
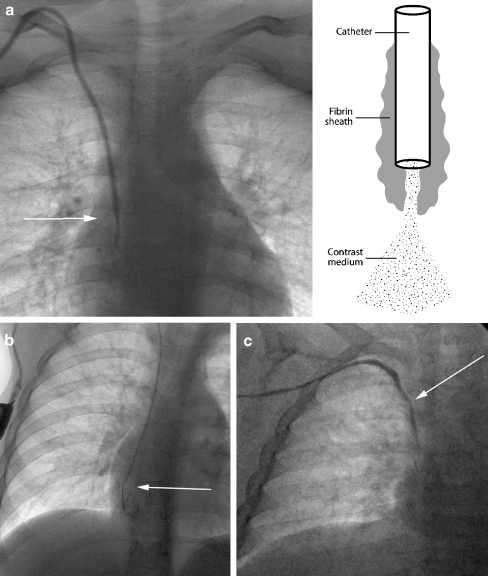
Fibrin sheaths. a Catheter contrast study in a 5-year-old male. Contrast medium exits the catheter tip in a linear manner, but the contrast jet is significantly narrower than the lumen of the catheter (arrow), implying the presence of a circumferential, nonocclusive fibrin sheath. The effect of the fibrin sheath is shown diagrammatically. b Contrast medium exits the tip of a portacath in an 11-year-old male. The jet fails to fan away from the tip (arrow) of the catheter, instead simply filling the lumen of the sheath. c A similar appearance is seen during a contrast study of a PICC in another patient. An arrow marks the catheter tip. Note the apparent irregular calibre of the catheter itself, a sign that contrast medium is tracking back along the catheter as shown in Fig. 21c
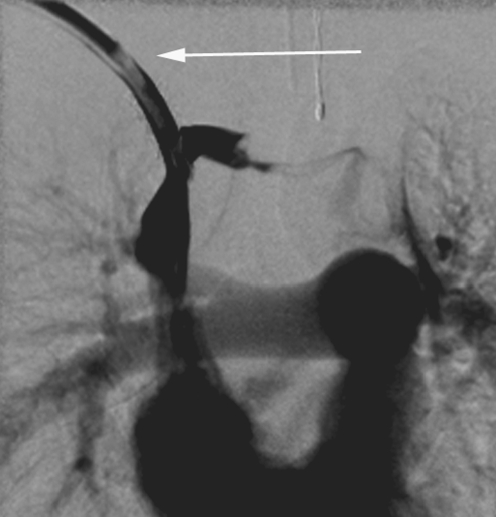
Image acquired during contrast medium injection through one lumen of a double-lumen catheter in a 2-year-old female. There is a filling defect within the catheter (arrow) at the site of a focal intraluminal thrombus
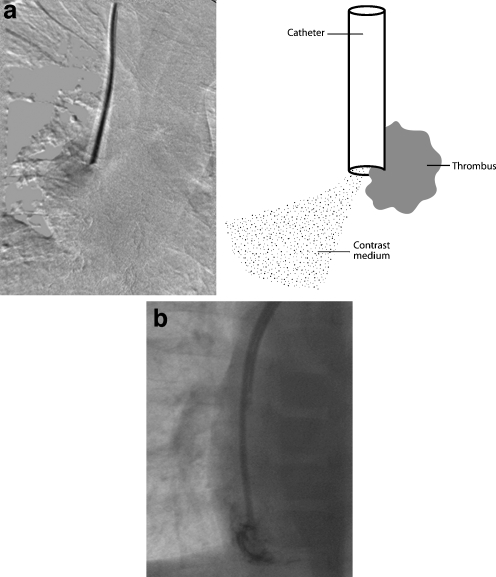
Thrombus. a Fluoroscopic image acquired during a catheter contrast study in a 3-year-old female. The contrast medium jet is deflected away from the long axis of the catheter, implying the presence of partially occlusive thrombus at the catheter tip. The effect of the tip thrombus is shown diagrammatically. b Thrombus is adherent to the tip of the distal lumen of a haemodialysis catheter in a 7-year-old male. Contrast medium exits the lumen eccentrically and outlines the thrombus
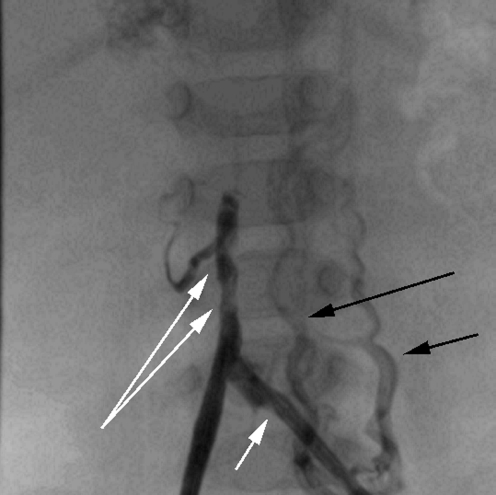
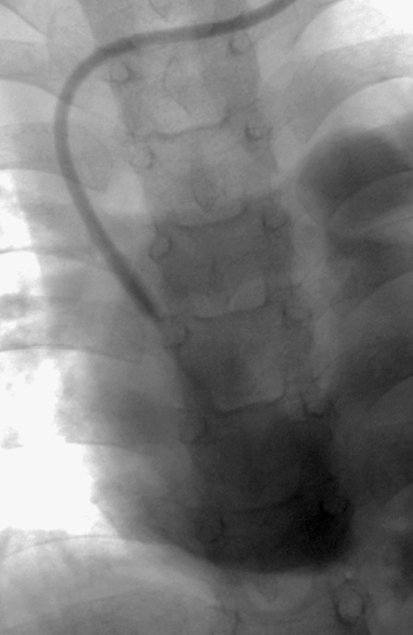
Contrast study of a left femoral catheter in a 7-month-old child. The short white arrow shows the tip of the catheter. Contrast medium outlines the common iliac veins and IVC. There are several filling defects in the IVC (long white arrows) consistent with venous thrombus beyond the catheter tip. Note that contrast medium also refluxes into ascending lumbar veins on the left (black arrows)

Left arm venography in a 1-year-old female with a malfunctioning tunnelled catheter in situ. Contrast medium fails to fill the occluded SVC and there are irregular filling defects within the left brachiocephalic vein, consistent with mural thrombi. Small collaterals are forming in the left supraclavicular region
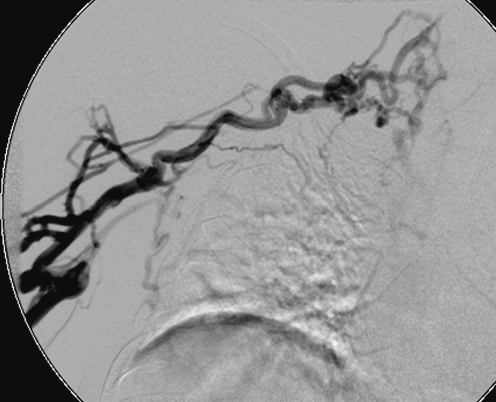
Right arm venogram in an 8-year-old boy performed prior to placement of a new catheter. The study demonstrates multiple irregular venous collaterals draining the arm following occlusion of the subclavian and brachiocephalic veins
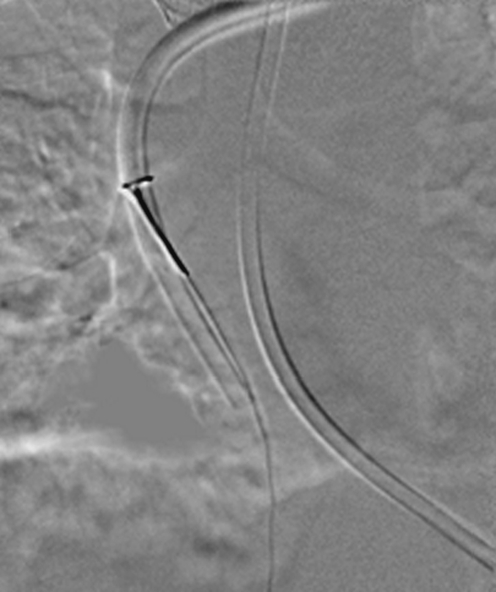
The distal portion of a malfunctioning haemodialysis catheter has been snared from a femoral approach in an attempt to strip the fibrin sheath from the catheter
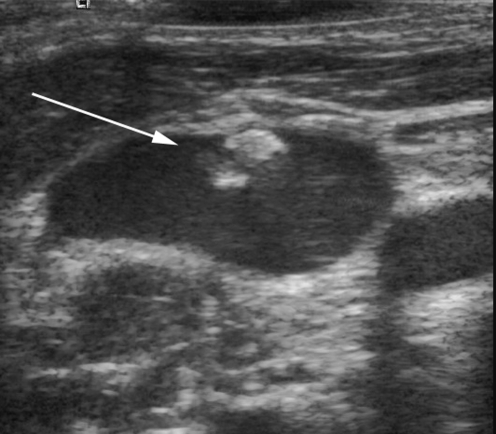
US image of the right internal jugular vein in a 12-year-old female. A linear filling defect is attached to the vessel wall (arrow), likely to represent a previous fibrin sheath in this patient with a history of multiple previous access catheters
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9114110', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9114110/'}]}
- Trerotola SO, Johnson MS, Harris VJ et al (1997) Outcome of tunneled hemodialysis catheters placed via the right internal jugular vein by interventional radiologists. Radiology 203:489–495 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '8425090', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8425090/'}]}
- Mauro MA, Jaques PF (1997) Radiologic placement of long-term central venous catheters: a review. J Vasc Interv Radiol 4:127–137 - PubMed
-
- None
- Rush J, Baskin KM, Cahill AM et al (2005) Central venous access by different service providers: does it matter who puts in the port? (abstract). Pediatr Radiol 35 [Suppl 1]:S76
-
- None
- Roebuck DJ, Kleidon TM, McLaren CA et al (2005) Internal jugular vein (IJV) patency after central venous (CV) access (abstract). Pediatr Radiol 35 [Suppl 1]:S75
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '10865606', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/10865606/'}]}
- Blum AS (1999) The role of the interventional radiologist in central venous access. J Intraven Nurs 22 [Suppl 6]:S32–S39 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
