

Measurement of the distribution of medial olivocochlear acoustic reflex strengths across normal-hearing individuals via otoacoustic emissions
- PMID: 17932717
- PMCID: PMC2538345
- DOI: 10.1007/s10162-007-0100-0
Measurement of the distribution of medial olivocochlear acoustic reflex strengths across normal-hearing individuals via otoacoustic emissions
Abstract
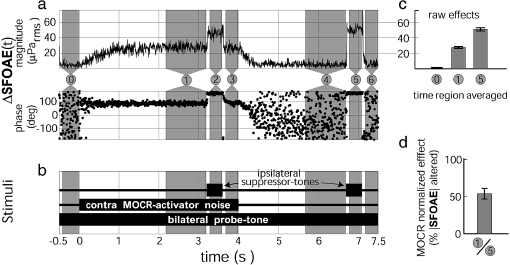
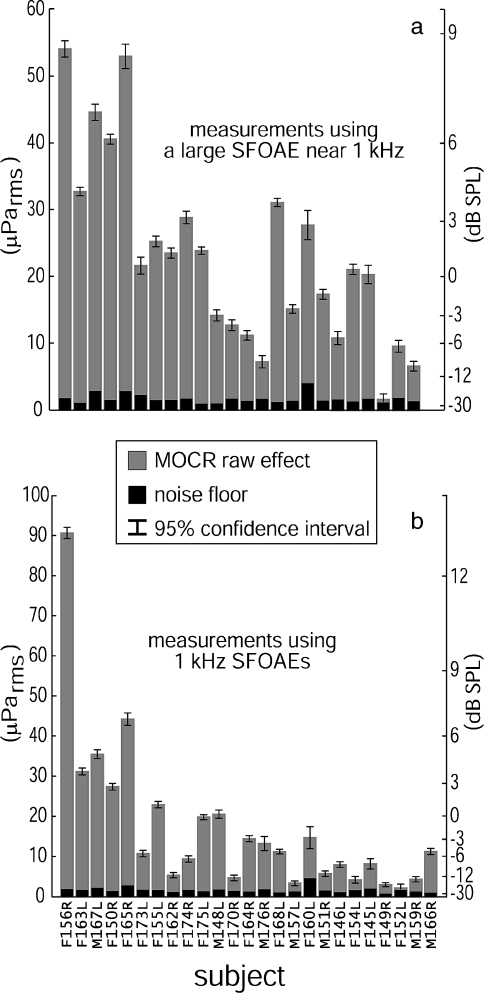
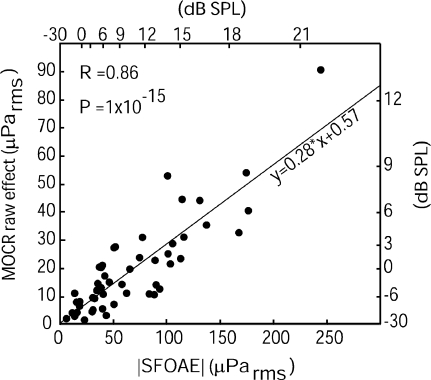
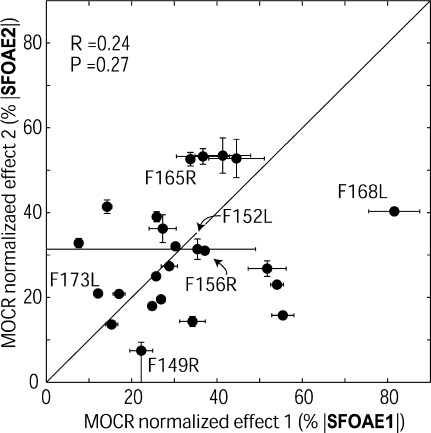
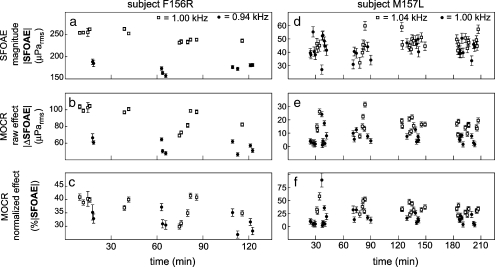
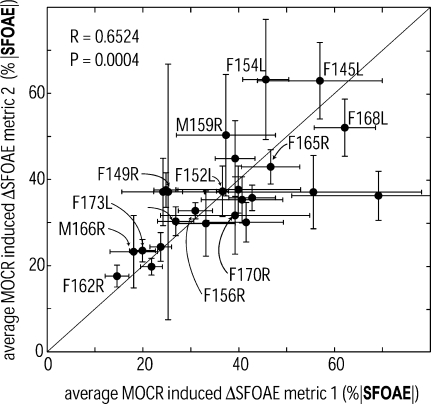
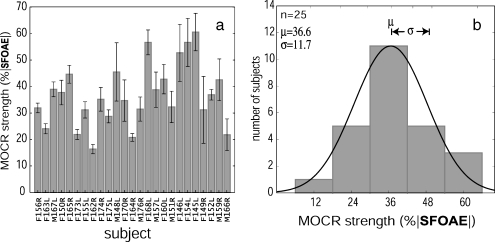
A clinical test for the strength of the medial olivocochlear reflex (MOCR) might be valuable as a predictor of individuals at risk for acoustic trauma or for explaining why some people have trouble understanding speech in noise. A first step in developing a clinical test for MOCR strength is to determine the range and variation of MOCR strength in a research setting. A measure of MOCR strength near 1 kHz was made across a normal-hearing population (N = 25) by monitoring stimulus-frequency otoacoustic emissions (SFOAEs) while activating the MOCR with 60 dB SPL wideband contralateral noise. Statistically significant MOCR effects were measured in all 25 subjects; but not all SFOAE frequencies tested produced significant effects within the time allotted. To get a metric of MOCR strength, MOCR-induced changes in SFOAEs were normalized by the SFOAE amplitude obtained by two-tone suppression. We found this "normalized MOCR effect" varied across frequency and time within the same subject, sometimes with significant differences between measurements made as little as 40 Hz apart or as little as a few minutes apart. Averaging several single-frequency measures spanning 200 Hz in each subject reduced the frequency- and time-dependent variations enough to produce correlated measures indicative of the true MOCR strength near 1 kHz for each subject. The distribution of MOCR strengths, in terms of SFOAE suppression near 1 kHz, across our normal-hearing subject pool was reasonably approximated by a normal distribution with mean suppression of approximately 35% and standard deviation of approximately 12%. The range of MOCR strengths spanned a factor of 4, suggesting that whatever function the MOCR plays in hearing (e.g., enhancing signal detection in noise, reducing acoustic trauma), different people will have corresponding differences in their abilities to perform that function.
Figures

References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1121/1.2434831', 'is_inner': False, 'url': 'https://doi.org/10.1121/1.2434831'}, {'type': 'PubMed', 'value': '17407896', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17407896/'}]}
- Backus BC. Bias due to noise in otoacoustic emission measurements. J. Acoust. Soc. Am. 121:1588–1603, 2007. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1121/1.2169918', 'is_inner': False, 'url': 'https://doi.org/10.1121/1.2169918'}, {'type': 'PubMed', 'value': '16708947', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16708947/'}]}
- Backus BC, Guinan JJ Jr. Time-course of the human medial olivocochlear reflex. J. Acoust. Soc. Am. 119:2889–2904, 2006. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.biopsych.2004.02.021', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.biopsych.2004.02.021'}, {'type': 'PubMed', 'value': '15158424', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15158424/'}]}
- Bar-Haim Y, Henkin Y, Ari-Even-Roth D, Tetin-Schneider S, Hildesheimer M, Muchnik C. Reduced auditory efferent activity in childhood selective mutism. Biol. Psychiatry 55:1061–1068, 2004. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00129492-200105000-00013', 'is_inner': False, 'url': 'https://doi.org/10.1097/00129492-200105000-00013'}, {'type': 'PubMed', 'value': '11347638', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11347638/'}]}
- De Ceulaer G, Yperman M, Daemers K, Van Driessche K, Somers T, Offeciers FE, Govaerts PJ. Contralateral suppression of transient evoked otoacoustic emissions: normative data for a clinical test set-up. Otol. Neurotol. 22:350–355, 2001. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1121/1.1903532', 'is_inner': False, 'url': 'https://doi.org/10.1121/1.1903532'}, {'type': 'PubMed', 'value': '4443490', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/4443490/'}]}
- Geisler CD. Letter: hypothesis on the function of the crossed olivocochlear bundle. J. Acoust. Soc. Am. 56:1908–1909, 1974. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
