

Collaborative communication in pediatric palliative care: a foundation for problem-solving and decision-making
- PMID: 17933613
- PMCID: PMC2151773
- DOI: 10.1016/j.pcl.2007.07.008
Collaborative communication in pediatric palliative care: a foundation for problem-solving and decision-making
Abstract
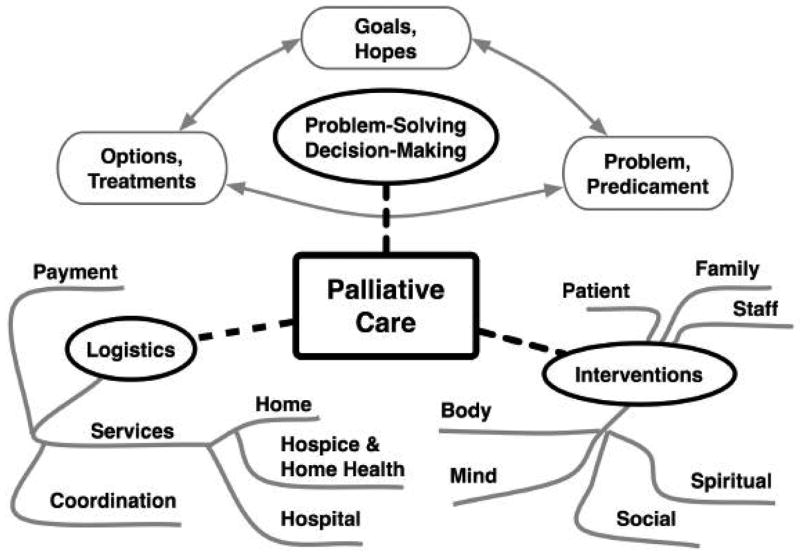
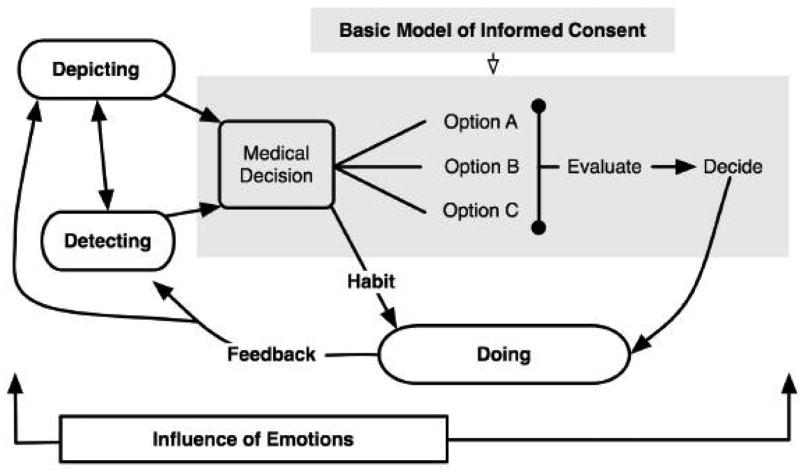
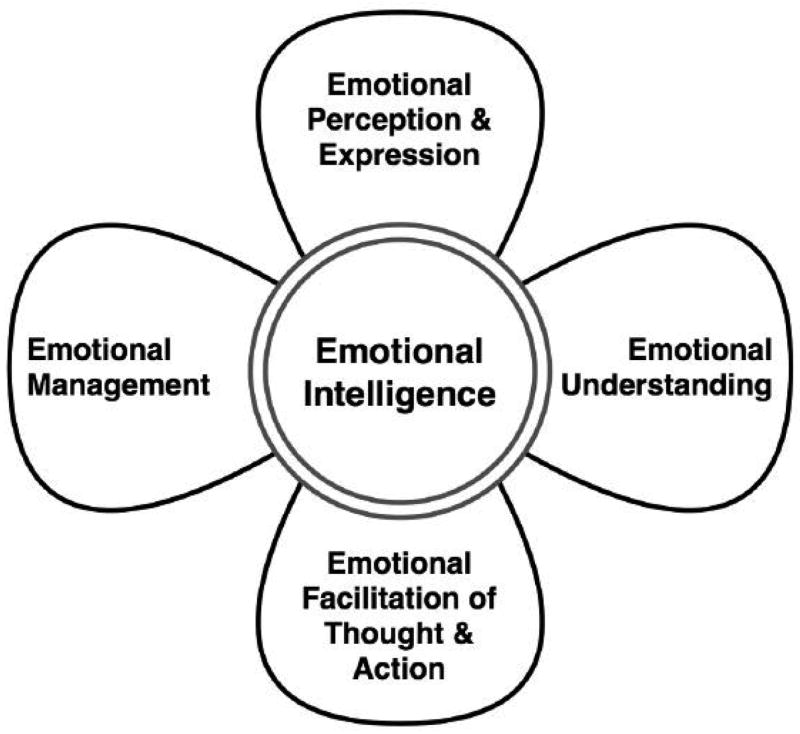
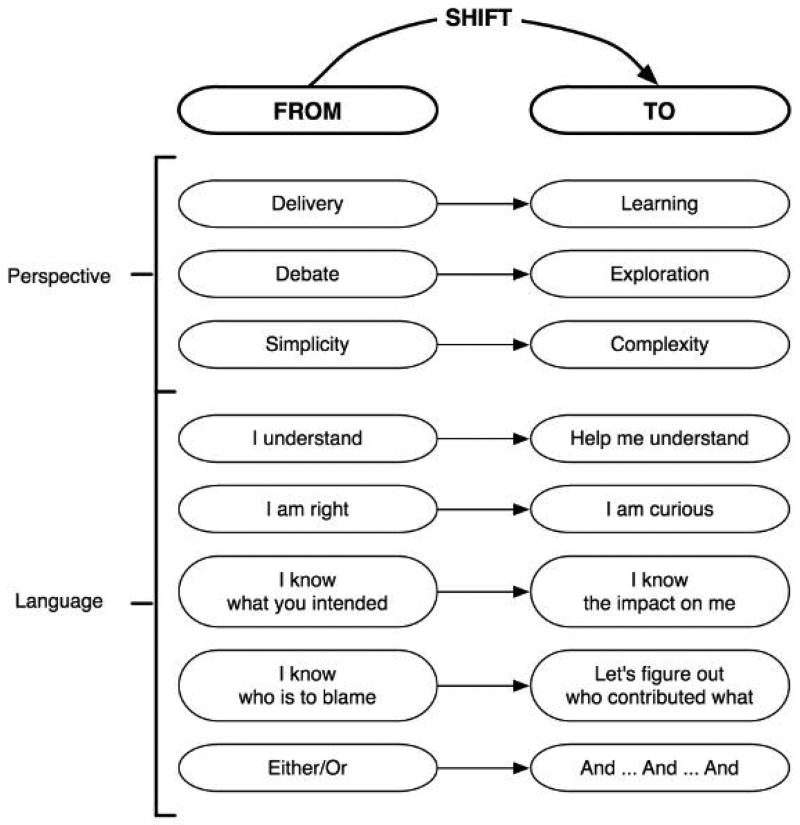
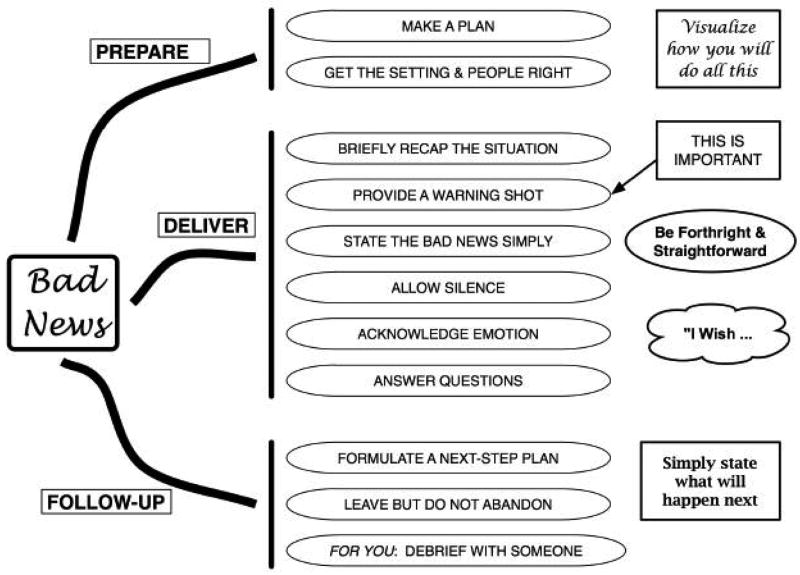
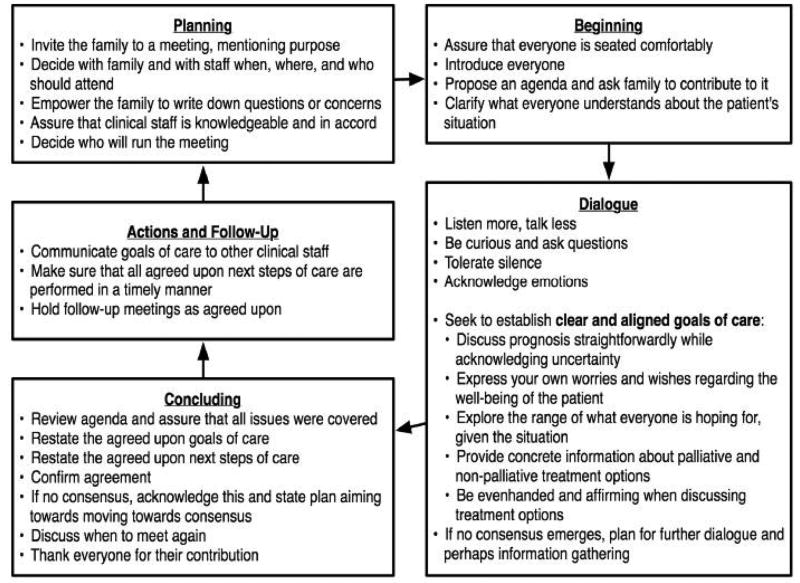
In an ideal world, all of us - patients, parents, family members, nurses, physicians, social workers, therapists, pastoral care workers, and others - would always work together in a collaborative manner to provide the best care possible. This article bases the framework for this ideal upon studies of communication between patients, families, and clinicians, as well as more general works on communication, collaboration, decision-making, mediation, and ethics, and is comprised of four parts: what is meant by collaborative communication; key concepts that influence how we frame the situations that children with life-threatening conditions confront and how these frameworks shape the care we provide; general topics that are important to the task of collaborative communication, specifically how we use heuristics when we set about to solve complicated problems; and three common tasks of collaborative communication, offering practical advice for patient care.
Figures
References
-
- Meyer EC, Ritholz MD, Burns JP, Truog RD. Improving the quality of end-of-life care in the pediatric intensive care unit: parents’ priorities and recommendations. Pediatrics. 2006;117(3):649–57. - PubMed
-
- Hays RM, Valentine J, Haynes G, Geyer JR, Villareale N, McKinstry B, et al. The Seattle Pediatric Palliative Care Project: effects on family satisfaction and health-related quality of life. J Palliat Med. 2006;9(3):716–28. - PubMed
-
- Back AL, Arnold RM. Dealing with conflict in caring for the seriously ill: “it was just out of the question”. JAMA. 2005;293(11):1374–81. - PubMed
-
- Katz J Johns Hopkins Paperbacks. The silent world of doctor and patient. Baltimore: Johns Hopkins University Press; 2002.
-
- Steinhauser KE, Christakis NA, Clipp EC, McNeilly M, McIntyre L, Tulsky JA. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284(19):2476–82. - PubMed
