

Serum procalcitonin and C-reactive protein concentrations to distinguish mildly infected from non-infected diabetic foot ulcers: a pilot study
- PMID: 17934713
- PMCID: PMC4749667
- DOI: 10.1007/s00125-007-0840-8
Serum procalcitonin and C-reactive protein concentrations to distinguish mildly infected from non-infected diabetic foot ulcers: a pilot study
Abstract
Aims/hypothesis: Infection of diabetic foot ulcers is common; at early stages it is difficult to differentiate between non-infected ulcers (or those colonised with normal flora) and ulcers infected with virulent bacteria that lead to deterioration. This pilot study aimed to assess the diagnostic accuracy of inflammatory markers as an aid to making this distinction.
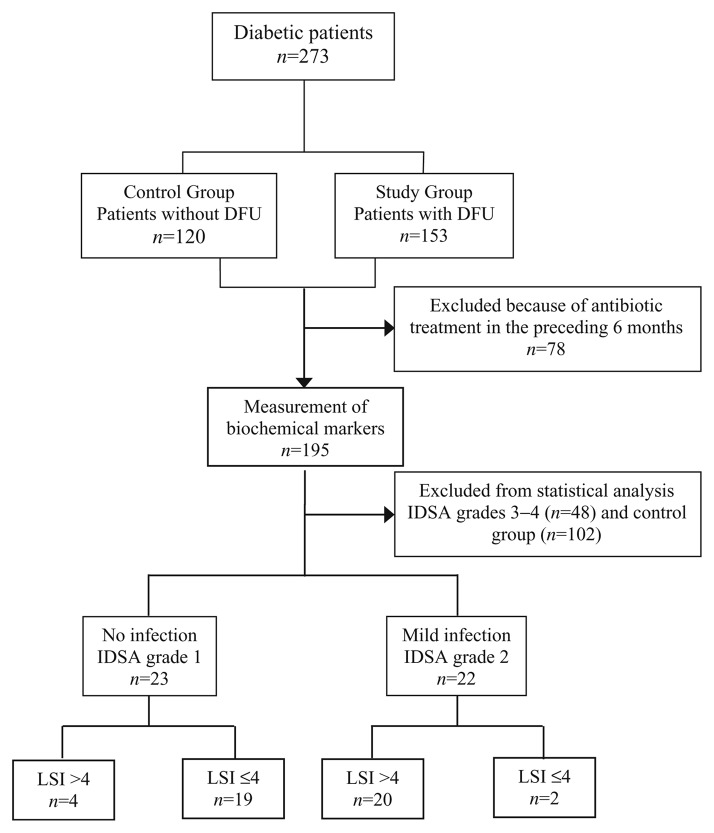
Methods: We included 93 diabetic patients who had an episode of foot ulcer and had not received antibiotics during the 6 months preceding the study. Ulcers were classified as infected or uninfected, according to the Infectious Diseases Society of America-International Working Group on the Diabetic Foot classification. Diabetic patients without ulcers (n=102) served as controls. C-reactive protein (CRP), orosomucoid, haptoglobin and procalcitonin were measured together with white blood cell and neutrophil counts. The diagnostic performance of each marker, in combination (using logistic regression) or alone, was assessed.
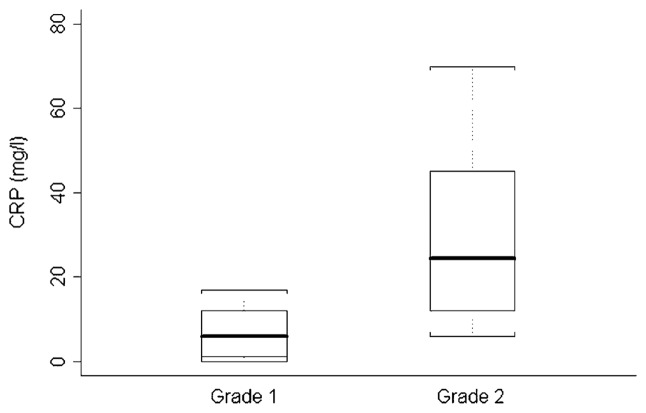
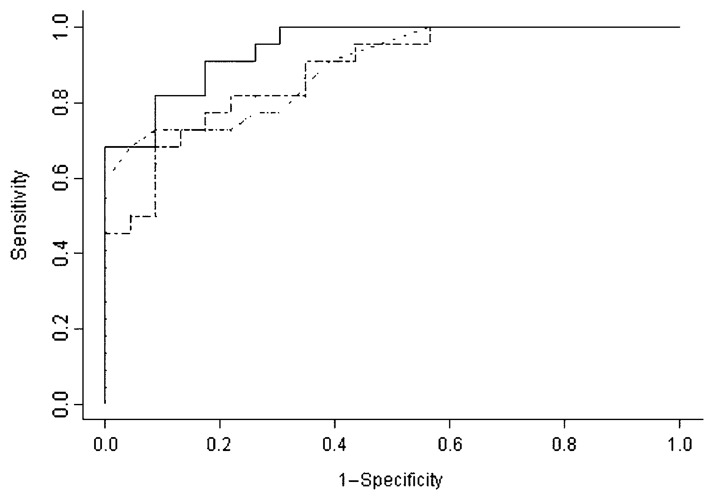
Results: As a single marker, CRP was the most informative for differentiating grade 1 from grade 2 ulcers (sensitivity 0.727, specificity 1.000, positive predictive value 1.000, negative predictive value 0.793) with an optimal cut-off value of 17 mg/l. In contrast, white blood cell and neutrophil counts were not predictive. The most relevant combination derived from the logistic regression was the association of CRP and procalcitonin (AUC 0.947), which resulted in a significantly more effective determination of ulcer grades, as shown by comparing receiver operating characteristic curves.
Conclusions/interpretation: Measurement of only two inflammatory markers, CRP and procalcitonin, might be of value for distinguishing between infected and non-infected foot ulcers in subgroups of diabetic patients, to help ensure the appropriate allocation of antibiotic treatment. Nevertheless, external validation of the diagnostic value of procalcitonin and CRP in diabetic foot ulcers is needed before routine use can be recommended.
Conflict of interest statement
Figures
Comment in
-
One small step for diabetic podopathy.Diabetologia. 2008 Feb;51(2):214-5. doi: 10.1007/s00125-007-0881-z. Diabetologia. 2008. PMID: 18030444 No abstract available.
Similar articles
-
Levels of wound calprotectin and other inflammatory biomarkers aid in deciding which patients with a diabetic foot ulcer need antibiotic therapy (INDUCE study).Diabet Med. 2018 Feb;35(2):255-261. doi: 10.1111/dme.13431. Epub 2017 Aug 15. Diabet Med. 2018. PMID: 28734103 Free PMC article.
-
Procalcitonin as a diagnostic aid in diabetic foot infections.Tohoku J Exp Med. 2007 Dec;213(4):305-12. doi: 10.1620/tjem.213.305. Tohoku J Exp Med. 2007. PMID: 18075234
-
Can procalcitonin predict bone infection in people with diabetes with infected foot ulcers? A pilot study.Diabetes Res Clin Pract. 2011 Oct;94(1):53-6. doi: 10.1016/j.diabres.2011.05.023. Epub 2011 Jun 11. Diabetes Res Clin Pract. 2011. PMID: 21658786
-
The efficacy of inflammatory markers in diagnosing infected diabetic foot ulcers and diabetic foot osteomyelitis: Systematic review and meta-analysis.PLoS One. 2022 Apr 27;17(4):e0267412. doi: 10.1371/journal.pone.0267412. eCollection 2022. PLoS One. 2022. PMID: 35476639 Free PMC article.
-
Usefulness of estimation of blood procalcitonin concentration versus C-reactive protein concentration and white blood cell count for therapeutic monitoring of sepsis in neonates.Postepy Hig Med Dosw (Online). 2014 Dec 21;68:1516-23. doi: 10.5604/17322693.1133101. Postepy Hig Med Dosw (Online). 2014. PMID: 25531715 Review.
Cited by
-
Incidence and association of ocular manifestations with the disease severity in COVID-19 patients of northern region of India.Taiwan J Ophthalmol. 2022 May 19;12(3):312-316. doi: 10.4103/tjo.tjo_12_22. eCollection 2022 Jul-Sep. Taiwan J Ophthalmol. 2022. PMID: 36248072 Free PMC article.
-
New insights in diabetic foot infection.World J Diabetes. 2011 Feb 15;2(2):24-32. doi: 10.4239/wjd.v2.i2.24. World J Diabetes. 2011. PMID: 21537457 Free PMC article.
-
Immune mediators in patients with acute diabetic foot syndrome.Diabetes Care. 2009 Aug;32(8):1491-6. doi: 10.2337/dc08-2318. Epub 2009 Jun 9. Diabetes Care. 2009. PMID: 19509015 Free PMC article.
-
Frequency of Ophthalmological Findings in Hospitalized COVID-19 Patients.Cureus. 2021 May 10;13(5):e14942. doi: 10.7759/cureus.14942. Cureus. 2021. PMID: 34123639 Free PMC article.
-
Erythrocyte sedimentation rate and C-reactive protein to monitor treatment outcomes in diabetic foot osteomyelitis.Int Wound J. 2017 Feb;14(1):142-148. doi: 10.1111/iwj.12574. Epub 2016 Mar 8. Int Wound J. 2017. PMID: 26953894 Free PMC article.
References
-
- Cavanagh PR, Lipsky BA, Bradbury AW, Botek G. Treatment for diabetic foot ulcers. Lancet. 2005;366:1725–1735. - PubMed
-
- Mayfield JA, Reiber GE, Sanders LJ, Janisse D, Pogach LM. Preventive foot care in people with diabetes. Diabetes Care. 1998;21:2161–2177. - PubMed
-
- Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005;336:1719–1724. - PubMed
-
- Lavery LA, Armstrong DG, Wunderlich RP, Mohler MJ, Wendel CS, Lipsky BA. Risk factors for foot infections in individuals with diabetes. Diabetes Care. 2006;29:1288–1293. - PubMed
-
- Frykberg RG, Zgonis T, Armstrong DG, et al. Diabetic foot disorders: a clinical practice guideline (2006 revision) J Foot Ankle Surg. 2006;45:S1–S66. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
