

The contribution of dental amalgam to urinary mercury excretion in children
- PMID: 17938746
- PMCID: PMC2022658
- DOI: 10.1289/ehp.10249
The contribution of dental amalgam to urinary mercury excretion in children
Abstract
Background: Urinary mercury concentrations are widely used as a measure of mercury exposure from dental amalgam fillings. No studies have evaluated the relationship of these measures in a longitudinal context in children.
Objective: We evaluated urinary mercury in children 8-18 years of age in relation to number of amalgam surfaces and time since placement over a 7-year course of amalgam treatment.
Methods: Five hundred seven children, 8-10 years of age at baseline, participated in a clinical trial to evaluate the neurobehavioral effects of dental amalgam in children. Subjects were randomized to either dental amalgam or resin composite treatments. Urinary mercury and creatinine concentrations were measured at baseline and annually on all participants.
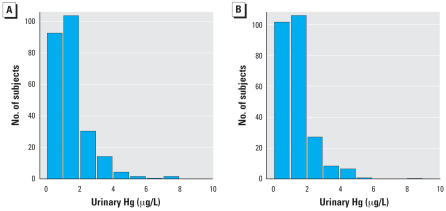
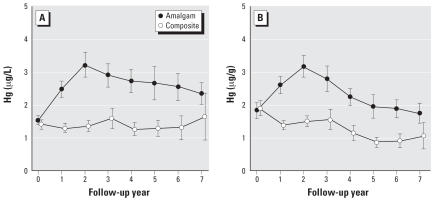
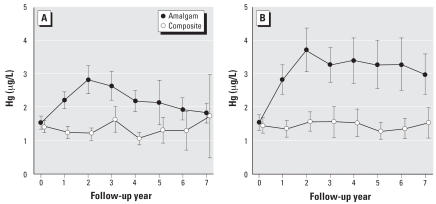
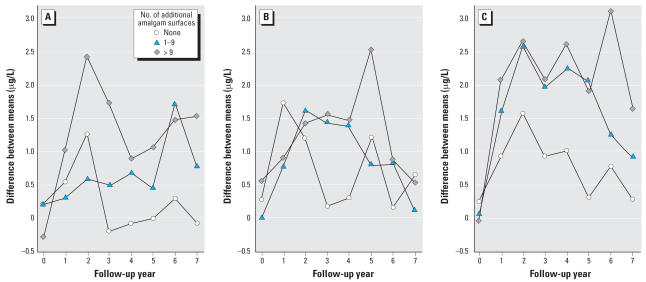
Results: Treatment groups were comparable in baseline urinary mercury concentration (approximately 1.5 microg/L). Mean urinary mercury concentrations in the amalgam group increased to a peak of approximately 3.2 microg/L at year 2 and then declined to baseline levels by year 7 of follow-up. There was a strong, positive association between urinary mercury and both number of amalgam surfaces and time since placement. Girls had significantly higher mean urinary mercury concentrations than boys throughout the course of amalgam treatment. There were no differences by race in urinary mercury concentration associated with amalgam exposure.
Conclusions: Urinary mercury concentrations are highly correlated with both number of amalgam fillings and time since placement in children. Girls excrete significantly higher concentrations of mercury in the urine than boys with comparable treatment, suggesting possible sex-related differences in mercury handling and susceptibility to mercury toxicity.
Keywords: amalgam; children; dental; mercury; urine.
Figures
Comment in
-
Contribution of dental amalgam to urinary mercury excretion in children.Environ Health Perspect. 2008 Mar;116(3):A107-8; author reply A108-9. doi: 10.1289/ehp.11013. Environ Health Perspect. 2008. PMID: 18335073 Free PMC article. No abstract available.
-
Urinary mercury levels in children with amalgam fillings.Environ Health Perspect. 2008 Jul;116(7):A286-A287. doi: 10.1289/ehp.11235. Environ Health Perspect. 2008. PMID: 18629336 Free PMC article. No abstract available.
Similar articles
-
Neurobehavioral effects of dental amalgam in children: a randomized clinical trial.JAMA. 2006 Apr 19;295(15):1784-92. doi: 10.1001/jama.295.15.1784. JAMA. 2006. PMID: 16622140 Clinical Trial.
-
Urinary porphyrin excretion in children with mercury amalgam treatment: findings from the Casa Pia Children's Dental Amalgam Trial.J Toxicol Environ Health A. 2009;72(14):891-6. doi: 10.1080/15287390902959557. J Toxicol Environ Health A. 2009. PMID: 19557617
-
Biomarkers of kidney integrity in children and adolescents with dental amalgam mercury exposure: findings from the Casa Pia children's amalgam trial.Environ Res. 2008 Nov;108(3):393-9. doi: 10.1016/j.envres.2008.07.003. Epub 2008 Aug 21. Environ Res. 2008. PMID: 18721920 Free PMC article.
-
Toxicological aspects on the release and systemic uptake of mercury from dental amalgam.Eur J Oral Sci. 1998 Apr;106(2 Pt 2):678-86. doi: 10.1046/j.0909-8836.1998.eos10602ii03.x. Eur J Oral Sci. 1998. PMID: 9584901 Review.
-
Mercury exposure from dental amalgam fillings: absorbed dose and the potential for adverse health effects.Crit Rev Oral Biol Med. 1997;8(4):410-36. doi: 10.1177/10454411970080040401. Crit Rev Oral Biol Med. 1997. PMID: 9391753 Review.
Cited by
-
Modification of neurobehavioral effects of mercury by a genetic polymorphism of coproporphyrinogen oxidase in children.Neurotoxicol Teratol. 2012 Sep-Oct;34(5):513-21. doi: 10.1016/j.ntt.2012.06.004. Epub 2012 Jul 2. Neurotoxicol Teratol. 2012. PMID: 22765978 Free PMC article. Clinical Trial.
-
Levels of Mercury in Fish-Eating Children, With and Without Amalgam Restoration.J Pharm Bioallied Sci. 2019 May;11(Suppl 2):S397-S401. doi: 10.4103/JPBS.JPBS_44_19. J Pharm Bioallied Sci. 2019. PMID: 31198376 Free PMC article.
-
Genetic polymorphisms affecting susceptibility to mercury neurotoxicity in children: summary findings from the Casa Pia Children's Amalgam clinical trial.Neurotoxicology. 2014 Sep;44:288-302. doi: 10.1016/j.neuro.2014.07.010. Epub 2014 Aug 7. Neurotoxicology. 2014. PMID: 25109824 Free PMC article.
-
Nephrotoxicity, neurotoxicity, and mercury exposure among children with and without dental amalgam fillings.Int J Hyg Environ Health. 2009 Jul;212(4):378-86. doi: 10.1016/j.ijheh.2008.09.004. Epub 2008 Nov 7. Int J Hyg Environ Health. 2009. PMID: 18996050 Free PMC article.
-
Genetic polymorphisms of catechol-O-methyltransferase modify the neurobehavioral effects of mercury in children.J Toxicol Environ Health A. 2014;77(6):293-312. doi: 10.1080/15287394.2014.867210. J Toxicol Environ Health A. 2014. PMID: 24593143 Free PMC article.
References
-
- Akesson I, Schutz A, Attewell R, Skerfving S, Glantz P-O. Status of mercury and selenium in dental personnel: impact of amalgam work and own fillings. Arch Environ Health. 1991;46:102–109. - PubMed
-
- Barregård L, Sällsten G, Schütz A, Attewell R, Skerfving S, Järvholm B. Kinetics of mercury in blood and urine after brief occupational exposure. Arch Environ Health. 1992;47:176–184. - PubMed
-
- Begerow J, Zander D, Freier I, Dunemann L. Long-term mercury excretion in urine after removal of amalgam fillings. Int Arch Occup Environ Health. 1994;66:209–212. - PubMed
-
- Bellinger DC, Trachtenberg T, Barregard L, Tavares M, Cernichiari E, Daniel D, et al. Neuropsychological and renal effects of dental amalgam in children: a randomized clinical trial. JAMA. 2006;295:1775–1783. - PubMed
-
- Berglund A, Pohl L, Olsson S, Bergman M. Determination of the rate of release of intra-oral mercury vapor from amalgam. J Dent Res. 1988;67:1235–1242. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
