

CXCL10/IP-10: a missing link between inflammation and anti-angiogenesis in preeclampsia?
- PMID: 17943641
- PMCID: PMC2396489
- DOI: 10.1080/14767050701483298
CXCL10/IP-10: a missing link between inflammation and anti-angiogenesis in preeclampsia?
Abstract
Objective: Interferon (IFN)-gamma inducible protein, CXCL10/IP-10, is a member of the CXC chemokine family with pro-inflammatory and anti-angiogenic properties. This chemokine has been proposed to be a key link between inflammation and angiogenesis. The aim of this study was to determine whether preeclampsia and delivery of a small for gestational age (SGA) neonate are associated with changes in maternal serum concentration of CXCL10/IP-10.
Study design: This cross-sectional study included patients in the following groups: (1) non-pregnant women (N = 49); (2) women with normal pregnancies (N = 89); (3) patients with preeclampsia (N = 100); and (4) patients who delivered an SGA neonate (N = 78). SGA was defined as birth weight below the 10th percentile. Maternal serum concentrations of CXCL10/IP-10 were measured by sensitive immunoassay. Non-parametric statistics were used for analysis.
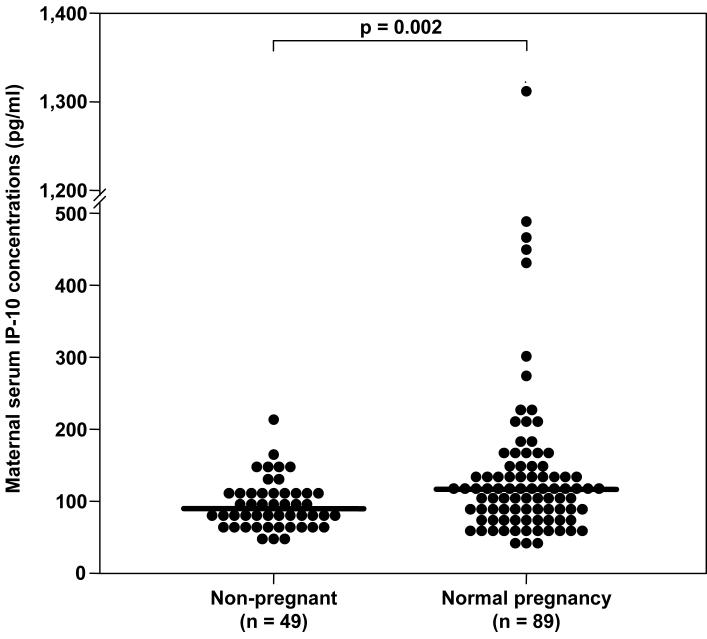
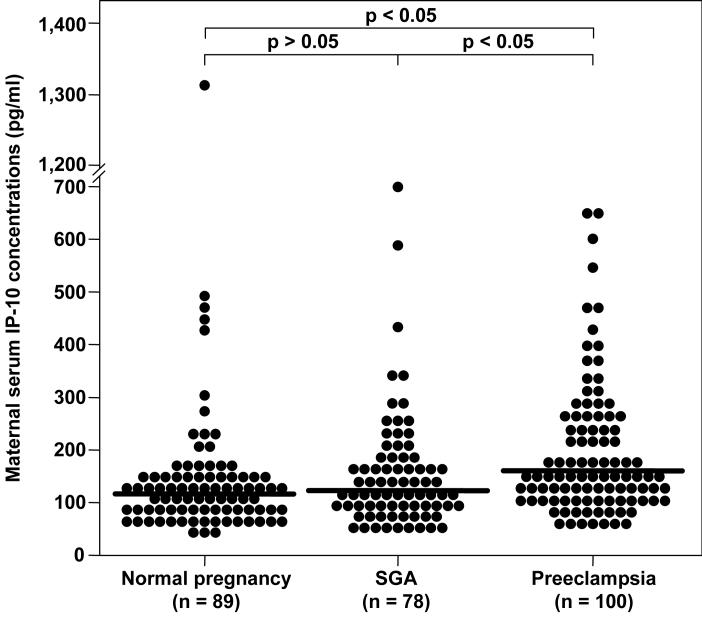
Results: (1) Patients with normal pregnancies had a significantly higher median serum concentration of CXCL10/IP-10 than non-pregnant women (median 116.1 pg/mL, range 40.7-1314.3 vs. median 90.3 pg/mL, range 49.2-214.7, respectively; p = 0.002); (2) no significant correlation was found between maternal serum concentration of CXCL10/IP-10 and gestational age (between 19 and 38 weeks); (3) there were no differences in median serum CXCL10/IP-10 concentrations between patients who delivered an SGA neonate and those with normal pregnancies (median 122.4 pg/mL, range 37.3-693.5 vs. median 116.1 pg/mL, range 40.7-1314.3, respectively; p > 0.05); (4) patients with preeclampsia had a higher median serum concentration of CXCL10/IP-10 than normal pregnant women (median 156.4 pg/mL, range 47.4-645.9 vs. median 116.1 pg/mL, range 40.7-1314.3, respectively; p < 0.05); (5) patients with preeclampsia had a higher median concentration of CXCL10/IP-10 than those who delivered an SGA neonate (median 156.4 pg/mL, range 47.4-645.9 vs. median 122.4 pg/mL, range 37.3-693.5, respectively; p < 0.05).
Conclusions: Patients with preeclampsia have significantly higher serum concentrations of CXCL10/IP-10 than both normal pregnant women and mothers who have SGA neonates. These results are likely to reflect an anti-angiogenic state as well as an enhanced systemic inflammatory response in patients with preeclampsia. Alternatively, since preeclampsia and SGA share several mechanisms of disease, it is possible that a higher concentration of this chemokine may contribute to the clinical presentation of preeclampsia in patients with a similar intrauterine insult.
Figures
Similar articles
-
Preeclampsia and small-for-gestational age are associated with decreased concentrations of a factor involved in angiogenesis: soluble Tie-2.J Matern Fetal Neonatal Med. 2008 Jun;21(6):389-402. doi: 10.1080/14767050802046069. J Matern Fetal Neonatal Med. 2008. PMID: 18570117 Free PMC article.
-
Maternal serum soluble CD30 is increased in normal pregnancy, but decreased in preeclampsia and small for gestational age pregnancies.J Matern Fetal Neonatal Med. 2007 Dec;20(12):867-78. doi: 10.1080/14767050701482993. J Matern Fetal Neonatal Med. 2007. PMID: 17853188 Free PMC article.
-
Maternal serum concentrations of the chemokine CXCL10/IP-10 are elevated in acute pyelonephritis during pregnancy.J Matern Fetal Neonatal Med. 2007 Oct;20(10):735-44. doi: 10.1080/14767050701511650. J Matern Fetal Neonatal Med. 2007. PMID: 17763275 Free PMC article.
-
Placental growth hormone is increased in the maternal and fetal serum of patients with preeclampsia.J Matern Fetal Neonatal Med. 2007 Sep;20(9):651-9. doi: 10.1080/14767050701463571. J Matern Fetal Neonatal Med. 2007. PMID: 17701665 Free PMC article.
-
Combined Anticoagulant Therapy for Prevention of Preeclampsia and Small for Gestational Age Neonates: A Systematic Review and Meta-analysis.Am J Perinatol. 2023 Dec;40(16):1745-1764. doi: 10.1055/a-1785-9032. Epub 2022 Mar 2. Am J Perinatol. 2023. PMID: 35235957
Cited by
-
Association between preeclampsia and the CXC chemokine family (Review).Exp Ther Med. 2015 May;9(5):1572-1576. doi: 10.3892/etm.2015.2337. Epub 2015 Mar 9. Exp Ther Med. 2015. PMID: 26136860 Free PMC article.
-
Placental Galectins Are Key Players in Regulating the Maternal Adaptive Immune Response.Front Immunol. 2019 Jun 19;10:1240. doi: 10.3389/fimmu.2019.01240. eCollection 2019. Front Immunol. 2019. PMID: 31275299 Free PMC article.
-
Pro-inflammatory profile of preeclamptic placental mesenchymal stromal cells: new insights into the etiopathogenesis of preeclampsia.PLoS One. 2013;8(3):e59403. doi: 10.1371/journal.pone.0059403. Epub 2013 Mar 19. PLoS One. 2013. PMID: 23527185 Free PMC article.
-
Maternal serum adiponectin multimers in preeclampsia.J Perinat Med. 2009;37(4):349-63. doi: 10.1515/JPM.2009.085. J Perinat Med. 2009. PMID: 19348608 Free PMC article.
-
Maternal and neonatal circulating visfatin concentrations in patients with pre-eclampsia and a small-for-gestational age neonate.J Matern Fetal Neonatal Med. 2010 Oct;23(10):1119-28. doi: 10.3109/14767050903572190. J Matern Fetal Neonatal Med. 2010. PMID: 20121389 Free PMC article.
References
-
- Brosens IA, Robertson WB, Dixon HG. The role of the spiral arteries in the pathogenesis of pre-eclampsia. J.Pathol. 1970;101:vi. - PubMed
-
- Brosens I, Dixon HG, Robertson WB. Fetal growth retardation and the arteries of the placental bed. Br.J.Obstet.Gynaecol. 1977;84:656–663. - PubMed
-
- De WF, Brosens I, Renaer M. Fetal growth retardation and the maternal arterial supply of the human placenta in the absence of sustained hypertension. Br.J.Obstet.Gynaecol. 1980;87:678–685. - PubMed
-
- Khong TY, De WF, Robertson WB, Brosens I. Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. Br.J.Obstet.Gynaecol. 1986;93:1049–1059. - PubMed
-
- Pijnenborg R, Anthony J, Davey DA, Rees A, Tiltman A, Vercruysse L, van AA. Placental bed spiral arteries in the hypertensive disorders of pregnancy. Br.J.Obstet.Gynaecol. 1991;98:648–655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources