

Trauma-associated lung injury differs clinically and biologically from acute lung injury due to other clinical disorders
- PMID: 17944012
- PMCID: PMC2765812
- DOI: 10.1097/01.ccm.0000280434.33451.87
Trauma-associated lung injury differs clinically and biologically from acute lung injury due to other clinical disorders
Abstract
Objective: Patients with trauma-associated acute lung injury have better outcomes than patients with other clinical risks for lung injury, but the mechanisms behind these improved outcomes are unclear. We sought to compare the clinical and biological features of patients with trauma-associated lung injury with those of patients with other risks for lung injury and to determine whether the improved outcomes of trauma patients reflect their baseline health status or less severe lung injury, or both.
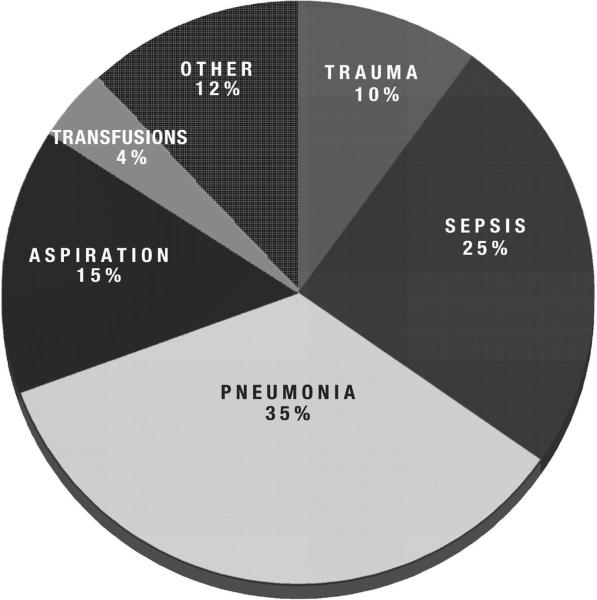
Design, setting, and patients: Analysis of clinical and biological data from 1,451 patients enrolled in two large randomized, controlled trials of ventilator management in acute lung injury.
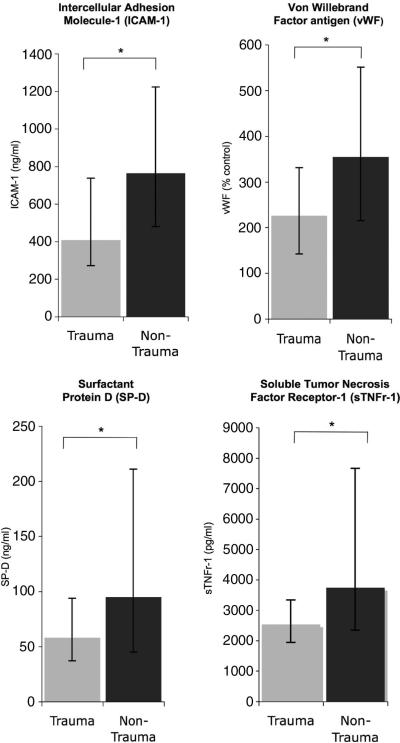
Measurements and main results: Compared with patients with other clinical risks for lung injury, trauma patients were younger and generally less acutely and chronically ill. Even after adjusting for these baseline differences, trauma patients had significantly lower plasma levels of intercellular adhesion molecule-1, von Willebrand factor antigen, surfactant protein-D, and soluble tumor necrosis factor receptor-1, which are biomarkers of lung epithelial and endothelial injury previously found to be prognostic in acute lung injury. In contrast, markers of acute inflammation, except for interleukin-6, and disordered coagulation were similar in trauma and nontrauma patients. Trauma-associated lung injury patients had a significantly lower odds of death at 90 days, even after adjusting for baseline clinical factors including age, gender, ethnicity, comorbidities, and severity of illness (odds ratio, 0.44; 95% confidence interval, 0.24-0.82; p = .01).
Conclusions: Patients with trauma-associated lung injury are less acutely and chronically ill than other lung injury patients; however, these baseline clinical differences do not adequately explain their improved outcomes. Instead, the better outcomes of the trauma population may be explained, in part, by less severe lung epithelial and endothelial injury.
(C) 2007 Lippincott Williams & Wilkins, Inc.
Figures
Comment in
-
The whole is greater than the sum of its parts.Crit Care Med. 2007 Oct;35(10):2431-2. doi: 10.1097/01.CCM.0000284487.28773.C0. Crit Care Med. 2007. PMID: 17885375 No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Wood KA, Huang D, Angus DC. Improving clinical trial design in acute lung injury. Crit Care Med. 2003;31(Suppl 4):S305–S311. - PubMed
-
- Eisner MD, Thompson T, Hudson LD, et al. Efficacy of low tidal volume ventilation in patients with different clinical risk factors for acute lung injury and the acute respiratory distress syndrome. Am J Respir Crit Care Med. 2001;164:231–236. - PubMed
-
- Stapleton RD, Wang BM, Hudson LD, et al. Causes and timing of death in patients with ARDS. Chest. 2005;128:525–532. - PubMed
-
- Hudson LD, Milberg JA, Anardi D, et al. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995;151(2 Pt 1):293–301. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
