

Improved survival of children with sepsis and purpura: effects of age, gender, and era
- PMID: 17945008
- PMCID: PMC2556765
- DOI: 10.1186/cc6161
Improved survival of children with sepsis and purpura: effects of age, gender, and era
Abstract
Background: To gain insight into factors that might affect results of future case-control studies, we performed an analysis of children with sepsis and purpura admitted to the paediatric intensive care unit (PICU) of Erasmus MC-Sophia Children's Hospital (Rotterdam, The Netherlands).
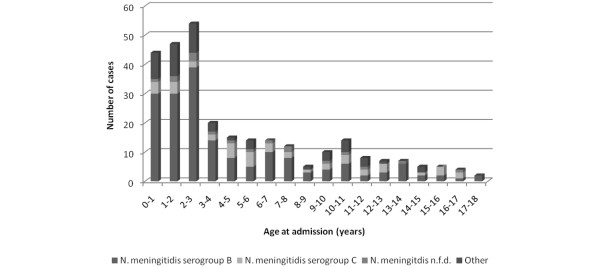
Methods: Between 1988 and 2006, all 287 children consecutively admitted with sepsis and purpura were included in various sepsis studies. Data regarding age, gender, ethnicity, serogroup of Neisseria meningitidis, severity, therapy, and survival were collected prospectively. These data were pooled into one database and analyzed retrospectively.
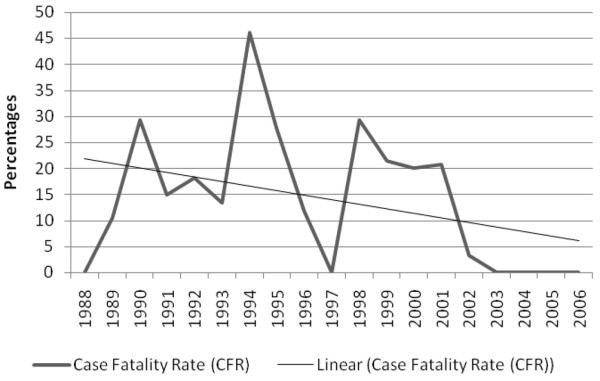
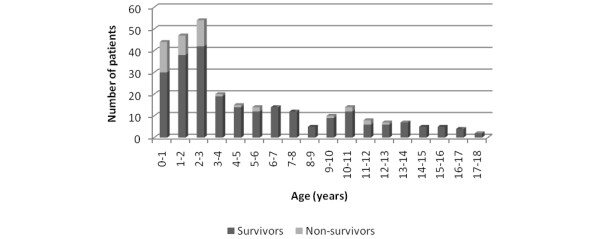
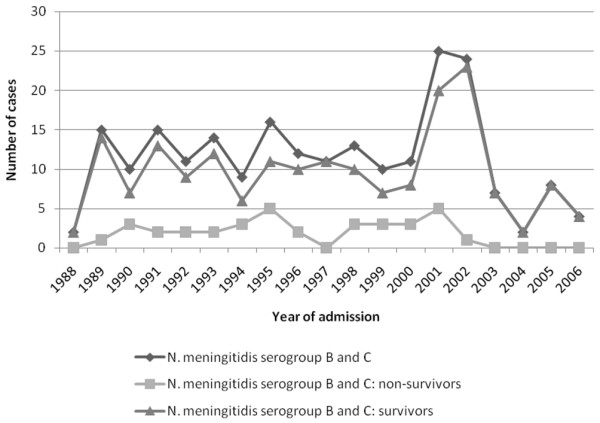
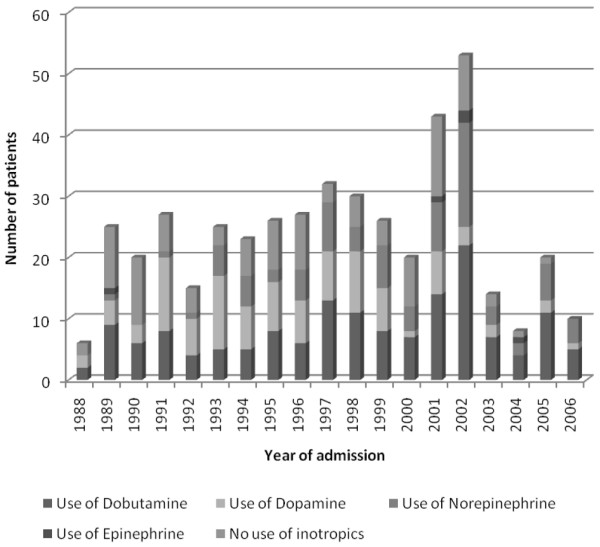
Results: The case fatality rate (CFR) from sepsis and purpura was 15.7%. During the study period, survival improved significantly. Younger age was significantly associated with more severe disease and a higher CFR. Children under the median age of 3.0 years had an increased risk of case fatality (odds ratio 4.3, 95% confidence interval 2.1 to 9.2; p < 0.001). Gender was not associated with CFR. However, males did have higher Paediatric Risk of Mortality scores, fewer PICU-free days, and more presence of shock. The course of sepsis and purpura was not related to ethnic origin. A causative organism was isolated in 84.3% of cases. N. meningitidis was the major organism (97.5%). Although N. meningitidis serogroup B was observed more often in younger children, serogroups were not associated with severity or survival. During the study period, the use of inotropic agents and corticosteroids changed substantially (less dopamine and more dobutamine, norepinephrine, and corticosteroids).
Conclusion: Age and gender are determinants of severity of paediatric sepsis and purpura. Survival rates have improved during the last two decades.
Figures
Comment in
-
Improvements in the outcome of children with meningococcal disease.Crit Care. 2007;11(5):172. doi: 10.1186/cc6140. Crit Care. 2007. PMID: 18001494 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
