

Immunohistochemical comparison of traditional and modified harvesting of the left internal mammary artery
- PMID: 17948077
- PMCID: PMC1995050
Immunohistochemical comparison of traditional and modified harvesting of the left internal mammary artery
Abstract
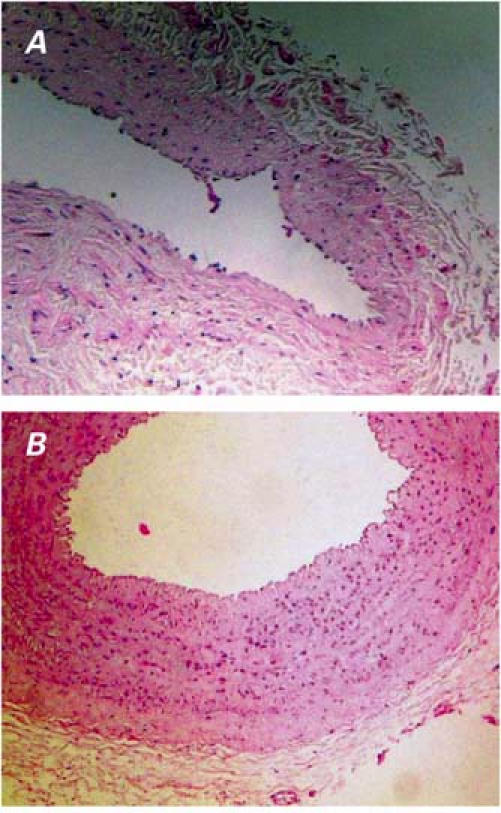
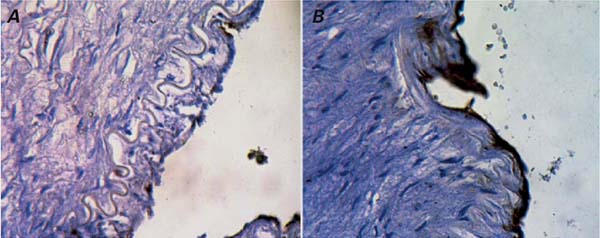
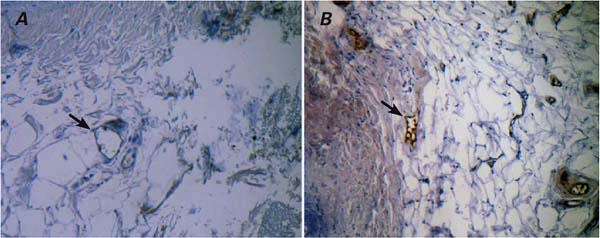
The left internal mammary artery is the conduit of choice for coronary artery bypass grafting. In the traditional ("clipped-artery") harvesting technique, this artery is prepared as a pedicle; the distal part is clipped, cut, and covered with a papaverine-soaked cloth until anastomosis is performed. In modified ("nonclipped-artery") harvesting, the prepared artery is kept in situ and left connected to the systemic circulation until anastomosis. Better outcomes from use of the nonclip technique have been reported. In order to determine comparative endothelial integrity and endothelial nitric oxide synthase activity, we performed an immunohistochemical study of arterial graft segments that were procured by each technique. This cross-sectional study involved 40 patients who underwent elective coronary artery bypass grafting. The patients were randomized into 2 groups of 20. One group underwent traditional clipped-artery harvesting; the other group, modified nonclipped-artery harvesting. By immunohistochemical methods, we examined redundant segments taken from bifurcation levels of the arteries. The tunica media was thinner in the clipped arterial segments, a phenomenon that we attribute to high luminal pressure. Endothelial nitric oxide synthase immunostaining was absent in regions of denudation in the luminal endothelia of the clipped arteries; in contrast, pronounced immunostaining occurred in the endothelia of the nonclipped segments. We found that traditional harvesting disrupted the integrity of the luminal endothelia of the clipped arteries. In addition, the traditional procedure decreased nitric oxide production, as was revealed by immunostaining.
Keywords: Coronary artery bypass/methods; coronary disease/surgery; endothelium, vascular/physiology; graft occlusion, vascular; graft survival; immunohistochemistry; internal mammary-coronary artery anastomosis/adverse effects/methods; mammary arteries/transplantation; myocardial revascularization/methods; nitric oxide synthase/analysis/metabolism/type III; tunica media/enzymology/pathology.
Figures
Similar articles
-
The comparison of traditional and modified harvesting techniques of left ınternal mammary artery regarding endothelin-1/2/3 expression and free flow capacity.J Cardiovasc Surg (Torino). 2015 Dec;56(6):913-8. Epub 2014 Mar 19. J Cardiovasc Surg (Torino). 2015. PMID: 24647318 Clinical Trial.
-
Unlocking vascular vitality: Exploring the impact of LIMA harvesting technique on endothelial health.Cardiovasc Pathol. 2025 Jan-Feb;74:107699. doi: 10.1016/j.carpath.2024.107699. Epub 2024 Sep 30. Cardiovasc Pathol. 2025. PMID: 39357782 Clinical Trial.
-
Localization of nitric oxide synthase type III in the internal thoracic and radial arteries and the great saphenous vein: a comparative immunohistochemical study.J Thorac Cardiovasc Surg. 2003 Jun;125(6):1510-5. doi: 10.1016/s0022-5223(03)00029-1. J Thorac Cardiovasc Surg. 2003. PMID: 12830073
-
[Endoscopic harvesting of internal mammary artery for coronary artery bypass grafting].Khirurgiia (Mosk). 2018;(11):96-99. doi: 10.17116/hirurgia201811196. Khirurgiia (Mosk). 2018. PMID: 30531763 Review. Russian.
-
Internal thoracic artery: anatomical and biological characteristics revisited.Asian Cardiovasc Thorac Ann. 2015 Jan;23(1):88-99. doi: 10.1177/0218492314523629. Epub 2014 Feb 11. Asian Cardiovasc Thorac Ann. 2015. PMID: 24585304 Review.
Cited by
-
All we need to know about internal thoracic artery harvesting and preparation for myocardial revascularization: a systematic review.J Cardiothorac Surg. 2021 Dec 27;16(1):354. doi: 10.1186/s13019-021-01733-2. J Cardiothorac Surg. 2021. PMID: 34961523 Free PMC article.
-
Human internal thoracic artery grafts exhibit severe morphological and functional damage and spasmic vasomotion due to oxidative stress.Med Sci Monit. 2011 Jul;17(7):CR411-6. doi: 10.12659/msm.881853. Med Sci Monit. 2011. PMID: 21709636 Free PMC article.
References
-
- Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med 1986;314:1–6. - PubMed
-
- Lytle BW, Loop FD, Cosgrove DM, Taylor PC, Goormastic M, Peper W, et al. Fifteen hundred coronary reoperations. Results and determinants of early and late survival. J Thorac Cardiovasc Surg 1987;93:847–59. - PubMed
-
- Grondin CM, Campeau L, Lesperance J, Enjalbert M, Bourassa MG. Comparison of late changes in internal mammary artery and saphenous vein grafts in two consecutive series of patients 10 years after operation. Circulation 1984;70(3 Pt 2):I208–12. - PubMed
-
- Fitzgibbon GM, Kafka HP, Leach AJ, Keon WJ, Hooper GD, Burton JR. Coronary bypass graft fate and patient outcome: angiographic follow-up of 5,065 grafts related to survival and reoperation in 1,388 patients during 25 years. J Am Coll Cardiol 1996;28:616–26. - PubMed
-
- Grondin CM, Campeau L, Thornton JC, Engle JC, Cross FS, Schreiber H. Coronary artery bypass grafting with saphenous vein. Circulation 1989;79(6 Pt 2):I24–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources