

doi: 10.1080/08998280.2007.11928329.
Bilateral neck swelling in a 40-year-old woman with HIV
Affiliations
- PMID: 17948114
- PMCID: PMC2014810
- DOI: 10.1080/08998280.2007.11928329
Item in Clipboard
Bilateral neck swelling in a 40-year-old woman with HIV
Proc (Bayl Univ Med Cent).
2007 Oct.
No abstract available
Figures

CT image of the upper neck shows innumerable pathologic, enlarged, low-density lymph nodes, which are characteristic (but not pathognomonic) for tuberculosis. Every nodal chain is involved, including retropharyngeal (arrowheads) and intraparotid (arrows) nodes.

CT image of the lower neck again shows similar pathologic nodes involving multiple nodal chains. The largest node (arrow) was aspirated and revealed acid-fast bacilli.

CT image of the chest with lung windows demonstrates an infiltrate within the anterior left upper lobe.

CT image of the upper abdomen demonstrates innumerable low-density lesions within the spleen (white arrows), consistent with microabscesses from disseminated tuberculosis. An abscess is present in the hepatic hilum (black arrow), and ascites is seen anterior to the liver (arrowhead).

CT image of the pelvis demonstrates characteristic pathologic bilateral iliac lymph nodes (arrows). Ascites is also seen in the pelvis (arrowhead).

Postprimary tuberculosis. CT image of the lungs demonstrates bronchiolar wall thickening (arrows) and mucoid impaction of contiguous branching bronchioles producing a tree-in-bud appearance (arrowheads). Tree-in-bud is characteristic, but not pathognomonic, for tuberculosis. Reprinted with permission from Radiographics (1).

Pott's disease. CT image of the spine demonstrates lytic destruction of the vertebral body (black arrow) with an adjoining soft-tissue abscess (white arrow). Reprinted with permission from Radiographics (1).

Ileal tuberculosis. There is irregularity and edema of the terminal ileum with marked narrowing of the lumen, as evidenced by the “string” of contrast (arrows). This appearance is nonspecific and there are many etiologies, with the most common being Crohn's disease. Reprinted with permission from Manpreet Singh Gulati, MD (5).

Renal tuberculosis. An ante-grade pyelogram shows characteristic calyceal dilation (long arrows) secondary to infundibular stenoses (short arrows). Proximal ureteral stricture (arrowhead) is also seen. Reprinted from Textbook of Uroradiology (6) with permission from Lippincott Williams & Wilkins.
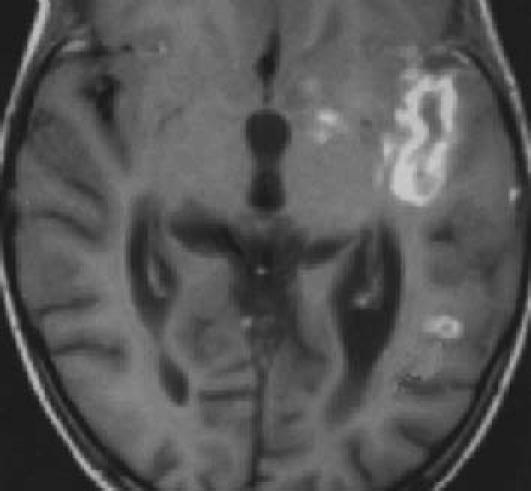
Central nervous system tuberculous meningitis. A postcontrast T1-weighted MR image demonstrates leptomeningeal enhancement along the left sylvian fissure (arrow). There is an accompanying ring-enhancing tuberculomain theleft parieto-occipital region (arrowhead). Reprinted with permission from Radiographics (1).

Artificial pneumothorax. (a) An apparatus from the 1930s, based on Forlaninis model. Reprinted courtesy of the Museu dHist ia de la Medicina de Catalunya. (b) Depiction of the procedure, designed to collapse the infected lung and allow it to “rest and heal.” This procedure was generally repeated every 10 to 15 days and lasted ver 3 to ears.

Plombage. A frontal chest radiograph demonstrates typical right-sided Lucite ball plombage. There is thinning and disorganization of the overlying ribs (arrow). Air-fluid levels in the Lucite balls (arrowheads) suggest bronchopleural fistulas. Reprinted with permission from Radiographics (1).

Countries with confirmed cases of extensively drug-resistant tuberculosis as of May 2007. The countries are Argentina, Armenia, Azerbaijan, Bangladesh, Brazil, Canada, Chile, China–Hong Kong SAR, Czech Republic, Ecuador, Estonia, France, Georgia, Germany, Ireland, Islamic Republic of Iran, Israel, Italy, Japan, Latvia, Lithuania, Mexico, Netherlands, Norway, Peru, Poland, Portugal, Republic of Korea, Romania, Russian Federation, Slovenia, South Africa, Spain, Sweden, Thailand, United Kingdom, and USA. Reprinted with permission from the World Health Organization.
Similar articles
-
A bilateral cervical swelling and it is not a malignancy.Oral Surg Oral Med Oral Pathol Oral Radiol. 2012 Jun;113(6):e19-21. doi: 10.1016/j.tripleo.2011.08.011. Epub 2012 Feb 17. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012. PMID: 22677025
-
[Unilateral eyelid swelling in naevus flammeus faciei. Problems in differential diagnosis of unilateral eyelid swelling].Hautarzt. 1994 Nov;45(11):792-8. doi: 10.1007/s001050050174. Hautarzt. 1994. PMID: 7822207 German.
-
A 69-year-old woman with periodic fever, facial swelling, and neck pain.Allergy Asthma Proc. 2018 Jul 1;39(4):322-325. doi: 10.2500/aap.2018.39.4139. Allergy Asthma Proc. 2018. PMID: 30095398
-
[A Case of HIV-associated Salivary Gland Disease (HSD) Presenting with Bilateral Parotid Abscesses].Nihon Jibiinkoka Gakkai Kaiho. 2016 Sep;119(9):1220-4. Nihon Jibiinkoka Gakkai Kaiho. 2016. PMID: 30035904 Review. Japanese.
-
Scrofuloderma: a forgotten disease?Skinmed. 2007 Nov-Dec;6(6):303-4. doi: 10.1111/j.1540-9740.2007.06607.x. Skinmed. 2007. PMID: 17975356 Review.
References
-
- Harisinghani MG, McLoud TC, Shepard JA, Ko JP, Shroff MM, Mueller PR. Tuberculosis from head to toe. Radiographics. 2000;20(2):449–470. - PubMed
-
- Perez-Solis D, Luyando LH, Callejo-Ortea A, Crespo-Hernandez M. Case 90: disseminated tuberculosis. Radiology. 2006;238(1):366–370. - PubMed
-
- Lucey BC, Stuhlfaut JW, Soto JA. Mesenteric lymph nodes seen at imaging: causes and significance. Radiographics. 2005;25(2):351–365. - PubMed
-
- Yang ZG, Min PQ, Sone S, He ZY, Liao ZY, Zhou XP, Yang GQ, Silverman PM. Tuberculosis versus lymphomas in the abdominal lymph nodes: evaluation with contrast-enhanced CT. AJR Am J Roentgenol. 1999;172(3):619–623. - PubMed
-
- All India Institute of Medical Sciences. The AIIMS Radiology Department abdominal tuberculosis imaging database Available at http://www.geocities.com/HotSprings/8093/abdtb.html; accessed July 15, 2007.
LinkOut - more resources
Full Text Sources