

The impact of the introduction of critical care outreach services in England: a multicentre interrupted time-series analysis
- PMID: 17949497
- PMCID: PMC2556766
- DOI: 10.1186/cc6163
The impact of the introduction of critical care outreach services in England: a multicentre interrupted time-series analysis
Abstract
Introduction: Critical care outreach services (CCOS) have been widely introduced in England with little rigorous evaluation. We undertook a multicentre interrupted time-series analysis of the impact of CCOS, as characterised by the case mix, outcome and activity of admissions to adult, general critical care units in England.
Methods: Data from the Case Mix Programme Database (CMPD) were linked with the results of a survey on the evolution of CCOS in England. Over 350,000 admissions to 172 units between 1996 and 2004 were extracted from the CMPD. The start date of CCOS, activities performed, coverage and staffing were identified from survey data and other sources. Individual patient-level data in the CMPD were collapsed into a monthly time series for each unit (panel data). Population-averaged panel-data models were fitted using a generalised estimating equation approach. Various potential outcomes reflecting possible objectives of the CCOS were investigated in three subgroups of admissions: all admissions to the unit, admissions from the ward, and unit survivors discharged to the ward. The primary comparison was between periods when a formal CCOS was and was not present. Secondary analyses considered specific CCOS activities, coverage and staffing.
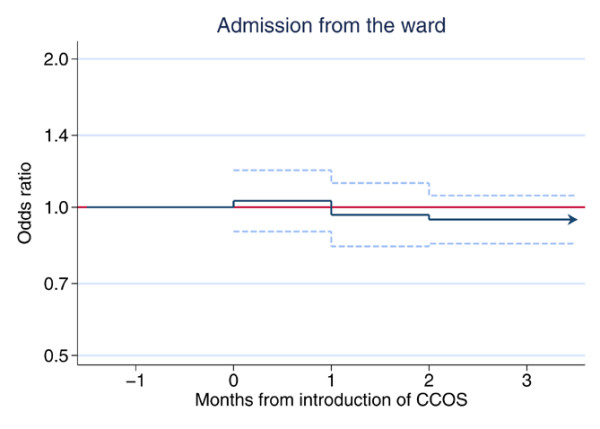
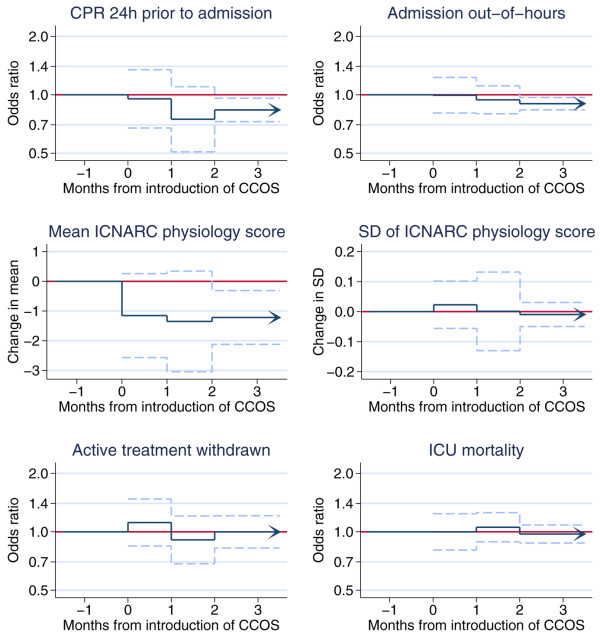
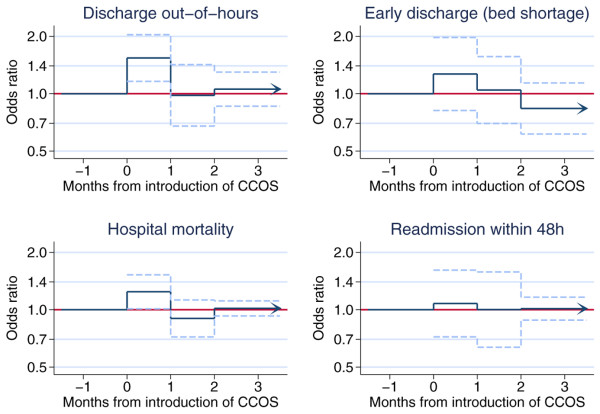
Results: In all, 108 units were included in the analysis, of which 79 had formal CCOS starting between 1996 and 2004. For admissions from the ward, CCOS were associated with significant decreases in the proportion of admissions receiving cardiopulmonary resuscitation before admission (odds ratio 0.84, 95% confidence interval 0.73 to 0.96), admission out of hours (odds ratio 0.91, 0.84 to 0.97) and mean Intensive Care National Audit & Research Centre physiology score (decrease in mean 1.22, 0.31 to 2.12). There was no significant change in unit mortality (odds ratio 0.97, 0.87 to 1.08) and no significant, sustained effects on outcomes for unit survivors discharged alive to the ward.
Conclusion: The observational nature of the study limits its ability to infer causality. Although associations were observed with characteristics of patients admitted to critical care units, there was no clear evidence that CCOS have a big impact on the outcomes of these patients, or for characteristics of what should form the optimal CCOS.
Figures
Comment in
-
The impact of critical care outreach: is there one?Crit Care. 2007;11(6):179. doi: 10.1186/cc6179. Crit Care. 2007. PMID: 18086323 Free PMC article. Review.
References
-
- Department of Health . Comprehensive Critical Care: a review of adult critical care services. London: Department of Health; 2000.
-
- Department of Health and NHS Modernisation Agency . The National Outreach Report 2003. London: Department of Health; 2003.
-
- Harrison DA, Brady AR, Rowan K. Case mix, outcome and length of stay for admissions to adult, general critical care units in England, Wales and Northern Ireland: the Intensive Care National Audit & Research Centre Case Mix Programme Database. Crit Care. 2004;8:R99–R111. doi: 10.1186/cc2834. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
