

Hyperdominant left anterior descending artery continuing across left ventricular apex as posterior descending artery coexistent with aortic stenosis
- PMID: 17949510
- PMCID: PMC2104526
- DOI: 10.1186/1749-8090-2-42
Hyperdominant left anterior descending artery continuing across left ventricular apex as posterior descending artery coexistent with aortic stenosis
Abstract
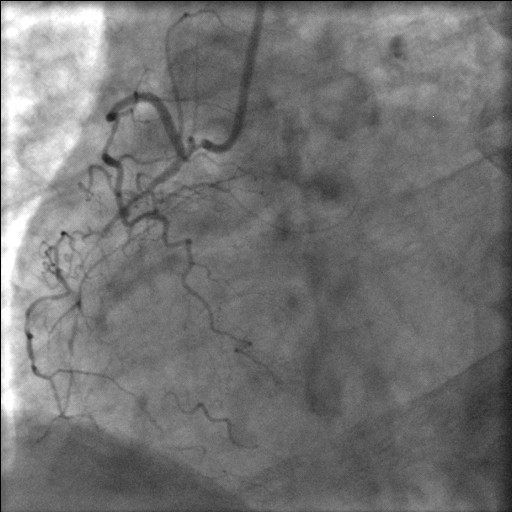
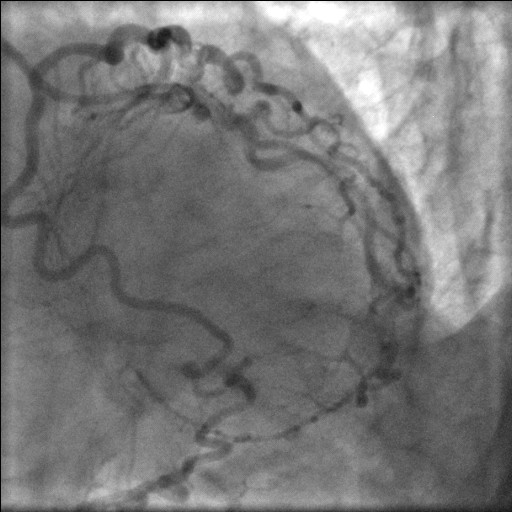
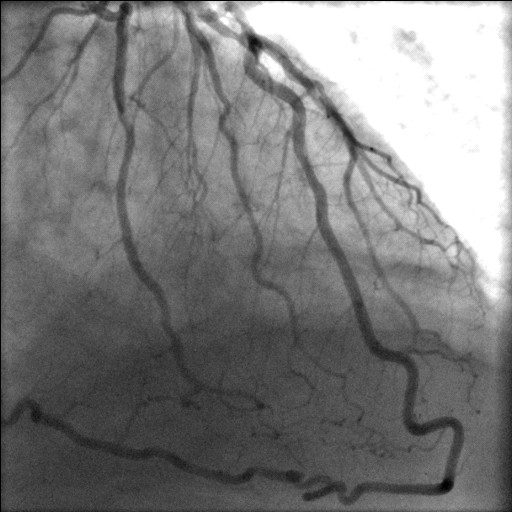
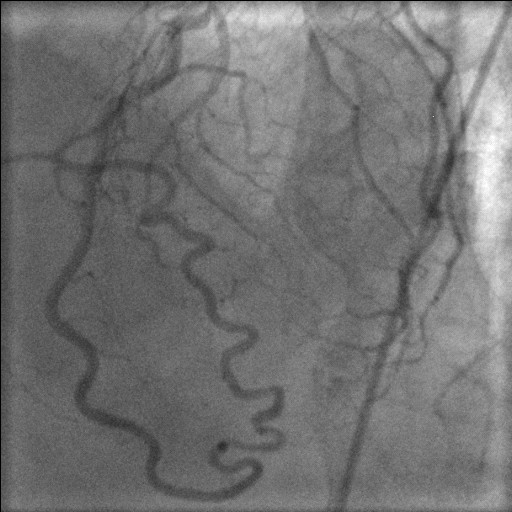
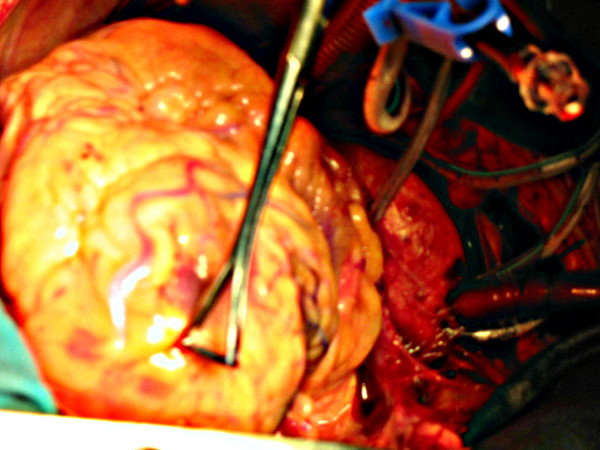
We describe, in a 61 year old man, with coexistent aortic stenosis, the anomalous origin of posterior descending artery (PDA) from a stenotic left anterior descending (LAD) artery, as its continuation across the left ventricular apex, in the presence of a normally arising and atretic proximal right coronary artery. The patient underwent mechanical aortic valve replacement and triple coronary artery bypass grafting and made an uneventful recovery. To the best of our knowledge, origin of PDA as a continuation of LAD across the left ventricular apex in the presence of a normally arising but atretic proximal right coronary artery has never been described in literature before. There is one previous case report of continuation of LAD as PDA across the left ventricular apex in a patient with single left coronary coronary artery with an absent right coronary ostium. As the blood supply to the entire interventricular septum is derived from this "hyperdominant" LAD system, stenosis of LAD can be catastrophic. A review of literature of the anomalies of right coronary artery and, in particular, of its anomalous origin from LAD and its coexistence with aortic stenosis, is presented.
Figures

References
-
- Click RL, Holmes DR, Jr, Vlietstra RE, Kosinski AS, Kronmal RA. Anomalous coronary arteries: location, degree of atherosclerosis and effect on survival – a report from the Coronary Artery Surgery Study. J Am Coll Cardiol. 1989;13:531–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
