

Impact of aging on the biology of breast cancer
- PMID: 17949989
- PMCID: PMC2626623
- DOI: 10.1016/j.critrevonc.2007.09.001
Impact of aging on the biology of breast cancer
Abstract
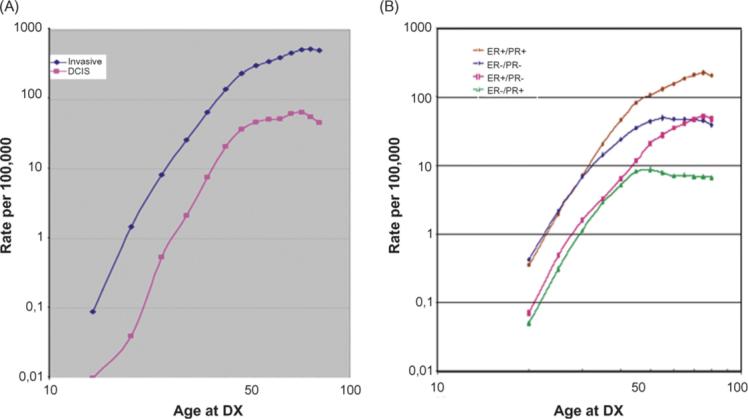
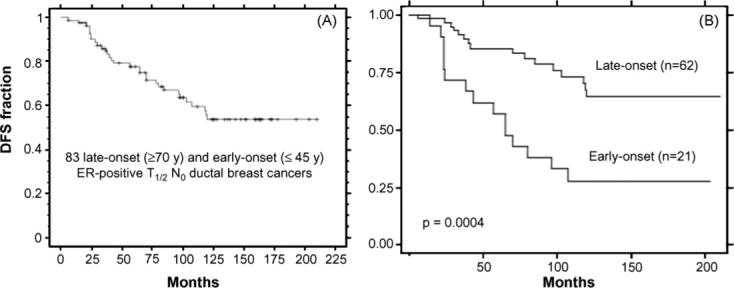
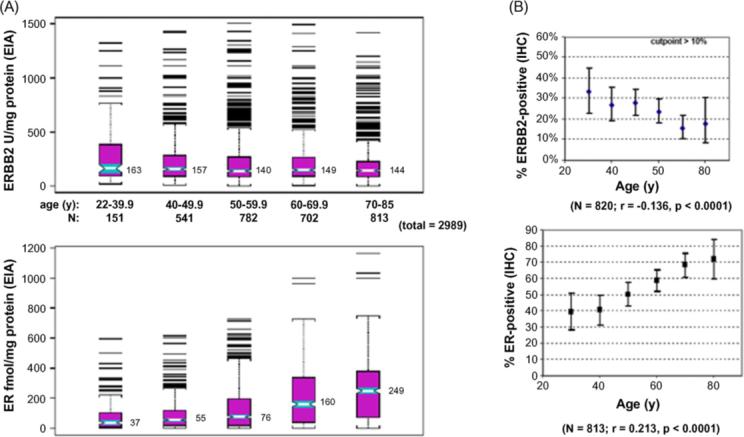
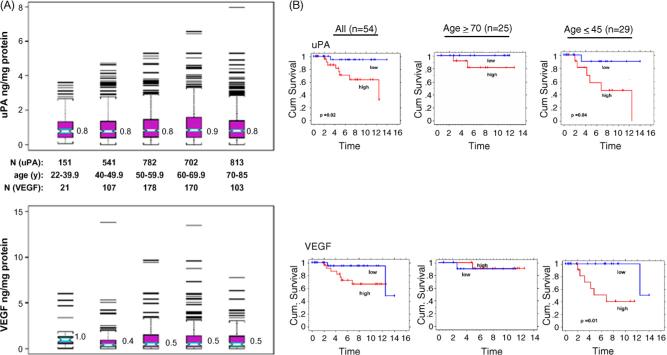
Breast cancer is a heterogeneous malignancy; its age-specific incidence profile rises exponentially until menopause and increases more slowly thereafter, reflecting the superimposition of early-onset and late-onset breast cancer rates. While early-onset breast cancers largely represent inherited or early life transforming effects on immature mammary epithelium, late-onset breast cancers likely follow extended exposures to promoting stimuli of susceptible epithelium that has failed to age normally. Among stimuli thought to promote late-onset breast tumorigenesis are the altered extracellular matrix and secreted products of senescent fibroblasts; however, the extent to which these senescent influences exist within the aging breast remains unknown. Clinical observations and biomarker studies indicate that late-onset breast cancers grow more slowly and are biologically less aggressive than early-onset breast cancers, even when controlled for hormone receptor (e.g. estrogen receptor, ER) and growth factor receptor (e.g. HER2) expression, supporting the conclusion that the biology of breast cancer is age-dependent.
Figures
References
-
- Thun MJ, Jemal A. Cancer epidemiology. In: Kufe DW, Bast RC, Hait WN, Hong WK, Pollock RE, Weichselbaum RR, Holland JF, Frei E III, editors. Cancer 7 medicine. BC Decker Inc.; Hamilton: 2006. pp. 339–53.
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- DevCan: Probability of developing or dying of cancer software. V6.1.0. 2006. Statistical Research and Applications Branch, National Cancer Institute ( http://www.srab.cancer.gov/devcan)
-
- Quong J, Eppenberger-Castori S, Moore D, III, et al. Age-dependent changes in breast cancer hormone receptors and oxidant stress markers. Breast Cancer Res Treat. 2002;76:221–36. - PubMed
-
- Anderson WF, Pfeiffer RM, Dores GM, Sherman ME. Comparison of age distribution patterns for different histopathologic types of breast cancer. Cancer Epidemiol Biomarkers Prev. 2006;15:1899–905. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
