

Intralesional injections of Citoprot-P (recombinant human epidermal growth factor) in advanced diabetic foot ulcers with risk of amputation
- PMID: 17953679
- PMCID: PMC7951380
- DOI: 10.1111/j.1742-481X.2007.00344.x
Intralesional injections of Citoprot-P (recombinant human epidermal growth factor) in advanced diabetic foot ulcers with risk of amputation
Abstract
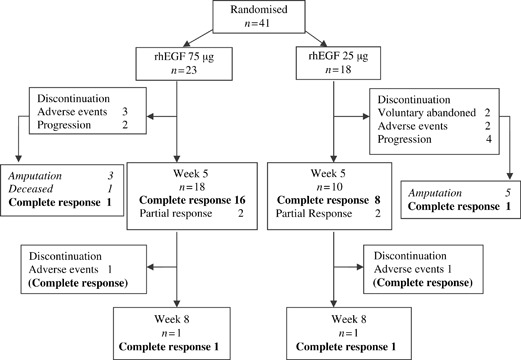
To investigate the efficacy and safety of recombinant human epidermal growth factor (rhEGF) in advanced diabetic foot ulcers (DFU) A double-blind trial was carried out to test two rhEGF dose levels in type 1 or 2 diabetes patients with Wagner's grade 3 or 4 ulcers, with high risk of amputation. Subjects were randomised to receive 75 (group I) or 25 mug (group II) rhEGF through intralesional injections, three times per week for 5-8 weeks together with standardised good wound care. Endpoints were granulation tissue formation, complete healing and need of amputation. Safety was assessed by clinical adverse events (AEs) and laboratory evaluations. Forty-one patients were included. After 5-8 weeks of treatment, 83% patients in the higher dose group and 61% in group II achieved useful granulation tissue covering more than 98% of the wound area. At long-term assessment, 13 (56.5%) patients healed in group I and 9 (50%) in group II. The mean time to complete healing in group I was 20.6 weeks (95% CI: 17.0-24.2) and 19.5 weeks (16.3-22.7) in group II. After 1-year follow-up, only one patient relapsed. Amputation was not necessary in 65% and 66.7% of groups I and II, respectively. The AEs rates were similar. The most frequent were sepsis (33%), burning sensation (29%), tremors, chills and local pain (25% each). rhEGF local injection enhances advanced DFU healing and reduces the risk of major amputation. No dose dependency was observed.
Figures
References
-
- Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047–53. - PubMed
-
- Frykberg RG, Armstrong DG, Giurini J, Edwards A, Kravete M, Kravitz S, Ross C, Stavosky J, Stuck R, Vanore J. Diabetic foot disorders. A clinical practice guideline. J Foot Ankle Surg 2000;39(5 Suppl):S1–S60. - PubMed
-
- Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, Hann AW, Hussein A, Jackson N, Johnson KE, Ryder CH, Torkington R, Van Ross ER, Whalley AM, Widdows P, Williamson S, Boulton AJ. The North‐West diabetes foot care study: incidence of, and risk factors for, new diabetic foot ulceration in a community‐based patient cohort. Diabet Med 2002;19:377–84. - PubMed
-
- Abbott CA, Vileikyte L, Williamson S, Carrington AL, Boulton AJM. Multicenter study of the incidence of and predictive risk factors for diabetic neuropathic foot ulceration. Diabetes Care 1998;21:1071–5. - PubMed
-
- Boulton AJ, Vileikyte L, Ragnarson‐Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet 2005;366:1719–24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
