

Flexor tendon and synovial gliding during simultaneous and single digit flexion in idiopathic carpal tunnel syndrome
- PMID: 17953971
- PMCID: PMC2254138
- DOI: 10.1016/j.jbiomech.2007.09.017
Flexor tendon and synovial gliding during simultaneous and single digit flexion in idiopathic carpal tunnel syndrome
Abstract
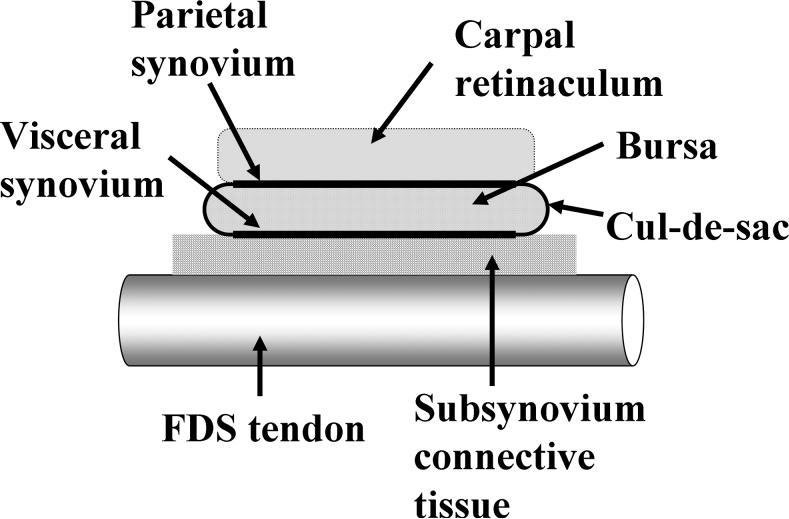
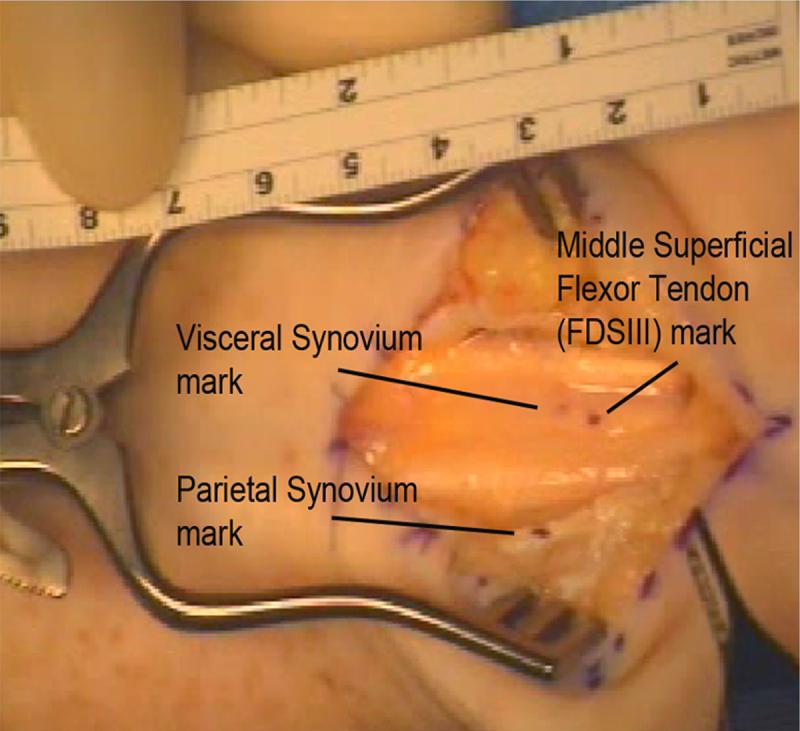
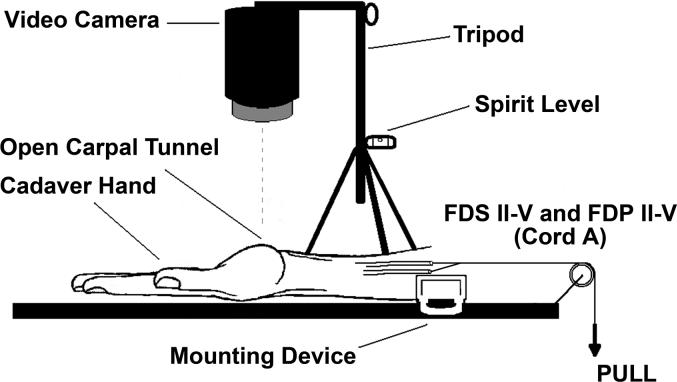
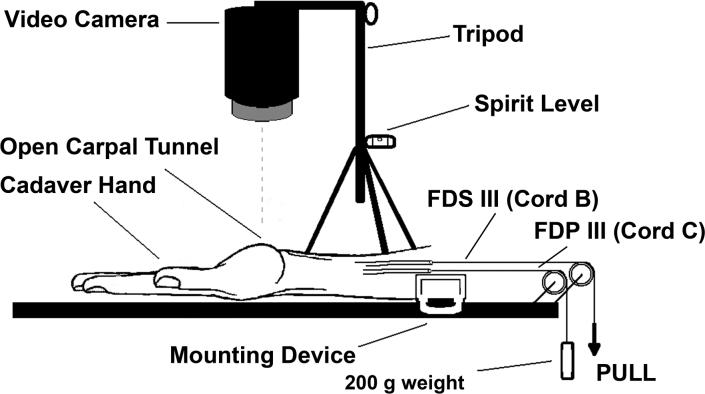
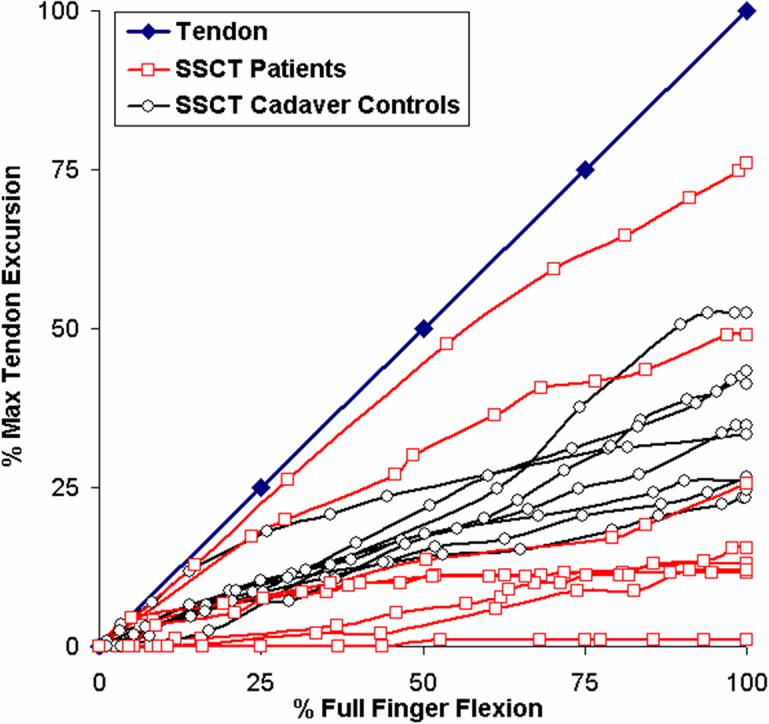
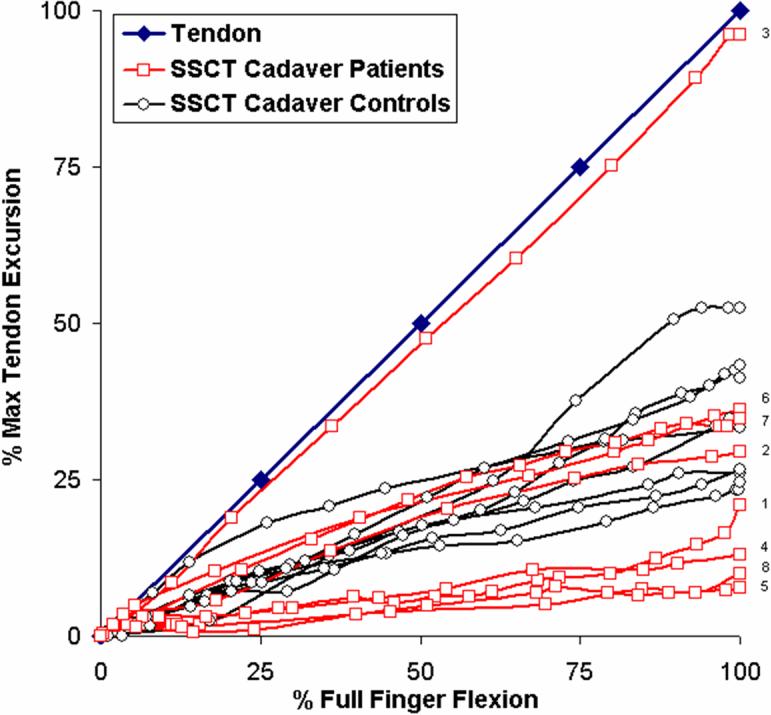
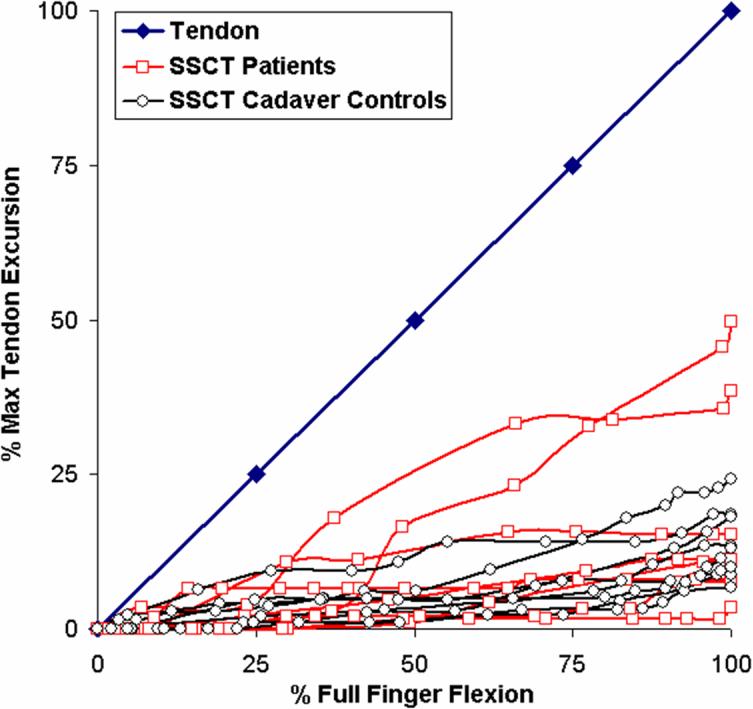
The characteristic pathological finding in carpal tunnel syndrome (CTS) is non-inflammatory fibrosis of the subsynovial connective tissue (SSCT), which lies between the flexor tendons and the visceral synovium (VS). How this fibrosis might affect tendon function is unknown. To better understand the normal function of the SSCT, the relative motion of the middle finger flexor digitorum superficialis (FDS III) tendon and VS was observed during finger flexion in patients with CTS and cadavers with a history of CTS and compared to normal cadavers. A digital camcorder was used to monitor the gliding motion of the FDS III tendon and SSCT in eight patients with idiopathic CTS undergoing carpal tunnel release surgery (CTR), in eight cadavers with an antemortem history of CTS and compared these with eight cadaver controls. There were no significant differences noted in the total movement of the SSCT relative to the FDS III. However, the pattern of SSCT movement relative to the FDS III in the CTS patients and cadavers with an antemortem history of CTS differed from the controls in one of two patterns, reflecting either increased SSCT adherence to FDS III or increased SSCT dissociation from FDS III. In CTS, the gliding characteristics of the SSCT are qualitatively altered. These changes may be the result of increased fibrosis within the SSCT, which in some cases has ruptured, resulting in SSCT-tendon dissociation. Similar changes are also identified postmortem in the CTS patient.
Figures
References
-
- AAEM Guidelines in electrodiagnostic medicine. American association of electrodiagnostic medicine. Muscle Nerve. 1992;15:229–253. - PubMed
-
- AAEM. AAN. AAPMR Practice parameter for electrodiagnostic studies in carpal tunnel syndrome: Summary statement. American association of electrodiagnostic medicine, american academy of neurology, american academy of physical medicine and rehabilitation. Muscle Nerve. 1993;16:1390–1391. - PubMed
-
- Abbas MA, Afifi AA, Zhang ZW, Kraus JF. Meta-analysis of published studies of work-related carpal tunnel syndrome. Int J Occup Environ Health. 1998;4:160–167. - PubMed
-
- Armstrong TJ, Castelli WA, Evans FG, Diaz-Perez R. Some histological changes in carpal tunnel contents and their biomechanical implications. J Occup Med. 1984;26:197–201. - PubMed
-
- Diao E, Shao F, Liebenberg E, Rempel D, Lotz JC. Carpal tunnel pressure alters median nerve function in a dose-dependent manner: A rabbit model for carpal tunnel syndrome. J Orthop Res. 2005;23:218–223. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
