

Hypertension after renal transplantation
- PMID: 17955265
- PMCID: PMC6904383
- DOI: 10.1007/s00467-007-0627-7
Hypertension after renal transplantation
Abstract
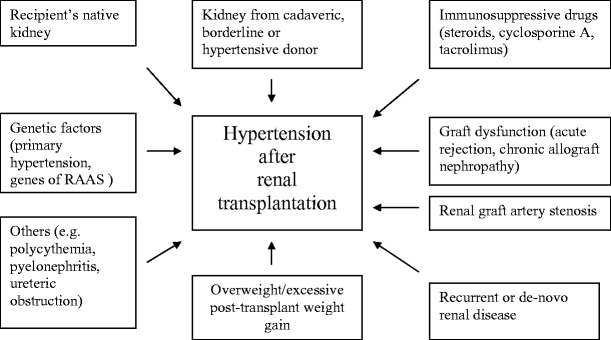
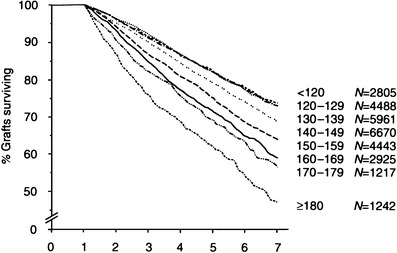
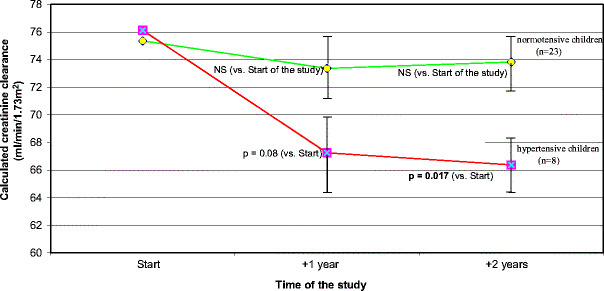
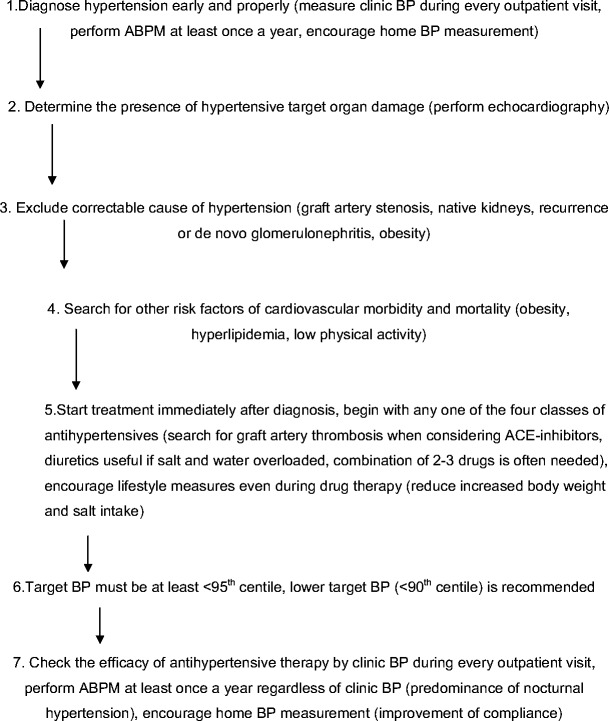
Hypertension is a common and serious complication after renal transplantation. It is an important risk factor for graft loss and morbidity and mortality of transplanted children. The etiology of posttransplant hypertension is multifactorial: native kidneys, immunosuppressive therapy, renal-graft artery stenosis, and chronic allograft nephropathy are the most common causes. Blood pressure (BP) in transplanted children should be measured not only by casual BP (CBP) measurement but also regularly by ambulatory BP monitoring (ABPM). The prevalence of posttransplant hypertension ranges between 60% and 90% depending on the method of BP measurement and definition. Left ventricular hypertrophy is a frequent type of end-organ damage in hypertensive children after transplantation (50-80%). All classes of antihypertensive drugs can be used in the treatment of posttransplant hypertension. Hypertension control in transplanted children is poor; only 20-50% of treated children reach normal BP. The reason for this poor control seems to be inadequate antihypertensive therapy, which can be improved by increasing the number of antihypertensive drugs. Improved hypertension control leads to improved long-term graft and patient survival in adults. In children, there is a great potential for antihypertensive treatment that could also result in improved graft and patient survival.
Figures
References
-
- Midtvedt K, Neumayer HH. Management strategies for posttransplant hypertension. Transplantation. 2000;70(Suppl 11):SS64–SS69. - PubMed
-
- Baluarte HJ, Gruskin AB, Ingelfinger JR, Stablein D, Tejani A. Analysis of hypertension in children post renal transplantation - a report of the North American Pediatric Renal Transplant Cooperative Study (NAPRTCS) Pediatr Nephrol. 1994;8:570–573. - PubMed
-
- Sorof JM, Sullivan EK, Tejani A, Portman RJ. Antihypertensive medication and renal allograft failure: A North American Pediatric Renal Transplant Cooperative Study report. J Am Soc Nephrol. 1999;10:1324–1330. - PubMed
-
- Kasiske BL, Guijarro C, Massy ZA, Wiederkehr MR, Ma JZ. Cardiovascular disease after renal transplantation. J Am Soc Nephrol. 1996;7:158–165. - PubMed
-
- Tutone VK, Mark PB, Stewart GA, Tan CC, Rodger RSC, Geddes CC, Jardine AG. Hypertension, antihypertensive agents and outcomes following renal transplantation. Clin Transplant. 2005;19:181–192. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
