

Lesion genesis in a subset of patients with multiple sclerosis: a role for innate immunity?
- PMID: 17956913
- PMCID: PMC2981817
- DOI: 10.1093/brain/awm236
Lesion genesis in a subset of patients with multiple sclerosis: a role for innate immunity?
Abstract
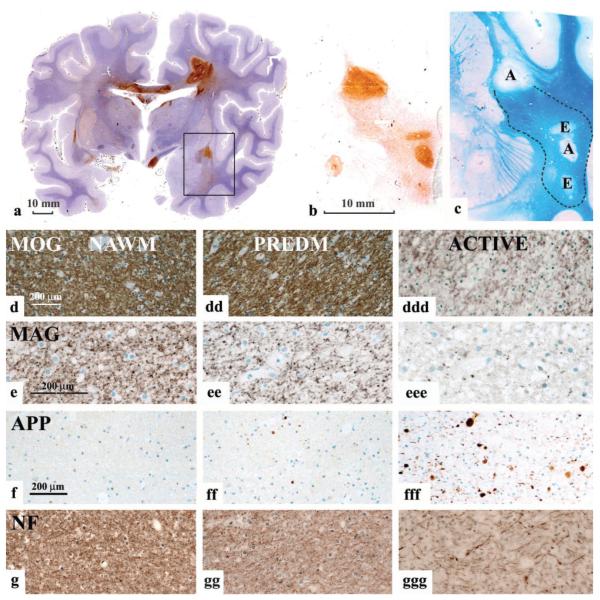
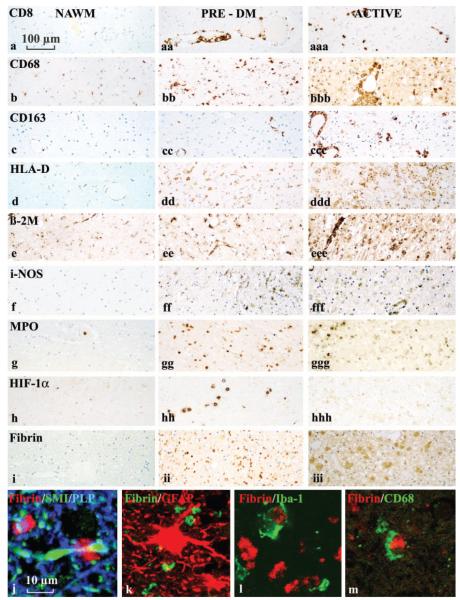
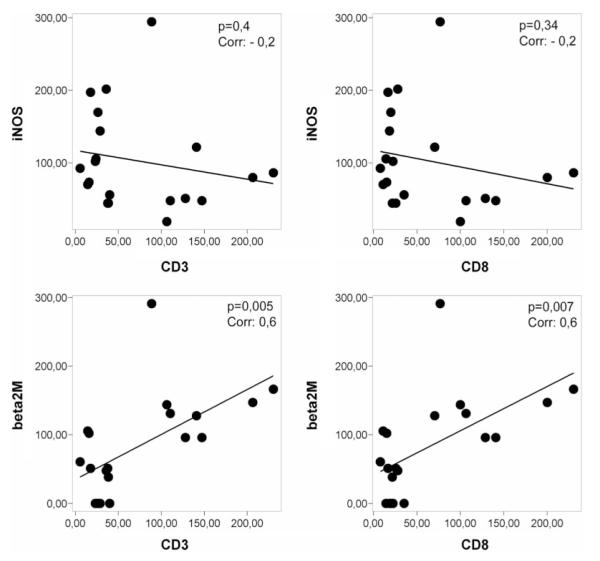
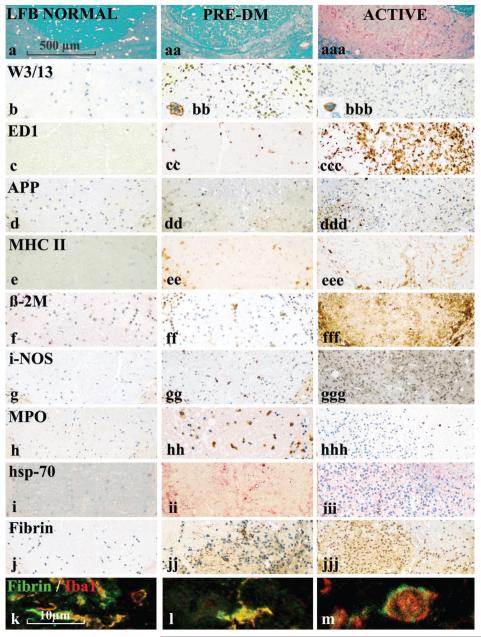
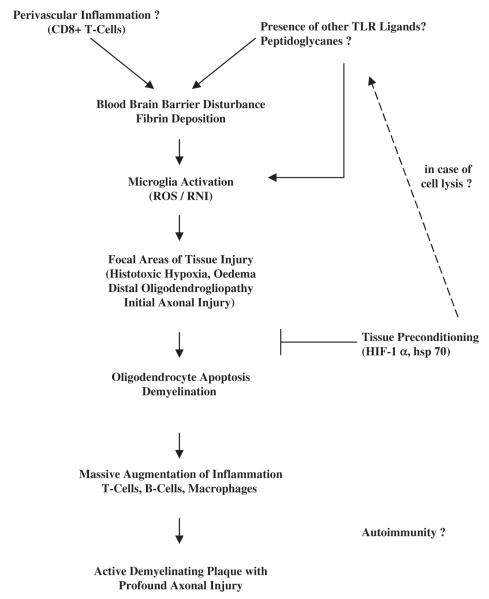
Lesions obtained early in the course of multiple sclerosis (MS) have been studied immunocytochemically, and compared with the early stages of the experimental lesion induced in rats by the intraspinal injection of lipopolysaccharide. Large hemispheric or double hemispheric sections were examined from patients who had died in the course of acute or early relapsing multiple sclerosis. In MS patients exhibiting hypoxia-like lesions [Pattern III; Lucchinetti et al. Ann Neurol (2000) 47: 707-17], focal areas in the white matter showed mild oedema, microglial activation and mild axonal injury in the absence of overt demyelination. In such lesions T-cell infiltration was mild and restricted to the perivascular space. Myeloperoxidase and the inducible form of nitric oxide synthase were expressed primarily by microglia, and the activated form of these cells was associated with extracellular deposition of precipitated fibrin. In addition, these lesions showed up-regulation of proteins involved in tissue preconditioning. When active demyelination started, lesions were associated with massive T-cell infiltration and microglia and macrophages expressed all activation markers studied. Similar tissue alterations were found in rats in the pre-demyelinating stage of lesions induced by the focal injection of bacterial lipopolysaccharide into the spinal white matter. We suggest that the areas of microglial activation represent an early stage of tissue injury, which precedes the formation of hypoxia-like demyelinated plaques. The findings indicate that mechanisms associated with innate immunity may play a role in the formation of hypoxia-like demyelinating lesions in MS.
Figures
Comment in
-
T cells and microglia as drivers of multiple sclerosis pathology.Brain. 2007 Nov;130(Pt 11):2755-7. doi: 10.1093/brain/awm246. Brain. 2007. PMID: 17956912 No abstract available.
References
-
- Aboul-Enein F, Rauschka H, Kornel B, Stadelmann C, Stefferl A, Brück W, et al. Preferential loss of myelin associated glycoprotein reflects hypoxialike white matter damage in stroke and inflammatory brain diseases. J Neuropath Exp Neurol. 2003;62:25–33. - PubMed
-
- Babinski J. Recherches sur l’anatomie pathologique de la sclerose en plaque et etude comparative des diverses varietes de la scleroses de la moelle. Arch Physiol (Paris) 1885;5–6:186–207.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
