

Modern management of obstructive salivary diseases
- PMID: 17957846
- PMCID: PMC2640028
Modern management of obstructive salivary diseases
Abstract
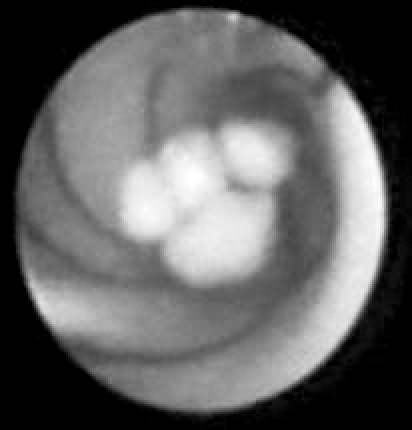
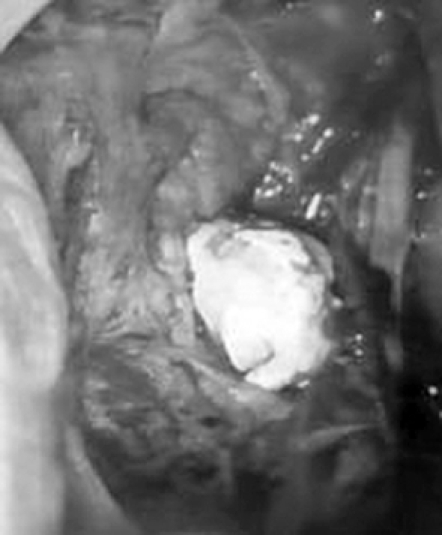
Over the last fifteen years, increasing public demand for minimally-invasive surgery and recent technological advances have led to the development of a number of conservative options for the therapeutic management of obstructive salivary disorders such as calculi and duct stenosis. These include extracorporeal shock-wave lithotripsy, sialoendoscopy, laser intra-corporeal lithotripsy, interventional radiology, the video-assisted conservative surgical removal of parotid and sub-mandibular calculi and botulinum toxin therapy. Each of these techniques may be used as a single therapeutic modality or in combination with one or more of the above-mentioned options, usually in day case or one-day case under local or general anaesthesia. The multi-modal approach is completely successful in about 80% of patients and reduces the need for gland removal in 3%, thus justifying the combination of, albeit, time-consuming and relatively expensive techniques as part of the modern and functional management of salivary calculi. With regard to the management of salivary duct anomalies, such as strictures and kinkings, interventional radiology with fluoroscopically controlled balloon ductoplasty seems to be the most suitable technique despite the use of radiation. Operative sialoendoscopy alone is the best therapeutic option for all mobile intra-luminal causes of obstruction, such as microliths, mucous plugs or foreign bodies, or for the local treatment of inflammatory conditions such as recurrent chronic parotitis or autoimmune salivary disorders. Finally, in the case of failure of one of the above techniques and regardless of the cause of obstruction, botulinum toxin injection into the parenchyma of the salivary glands using colour Doppler ultrasonographic monitoring should be considered before deciding on surgical gland removal.
Negli ultimi quindici anni la sempre maggiore richiesta di terapie minimamente invasive ed i recenti progressi tecnologici hanno favorito l’affermazione di tecniche conservative nel management dei disordini ostruttivi salivari quali la scialolitiasi e le stenosi duttali. Tali nuove opzioni terapeutiche includono la litotrissia extracorporea, l’endoscopia salivare, la litotrissia intracorporea laser, la radiologia interventistica, la rimozione chirurgica di calcoli parotidei e sottomandibolari video-assistita con preservazione ghiandolare ed il trattamento con tossina botulinica. Le tecniche menzionate possono essere impiegate singolarmente oppure combinate tra loro, generalmente in regime ambulatoriale o di Day Surgery e One-Day Surgery in anestesia locale o generale. L’elevato successo terapeutico, pari a circa l’80%, garantito dall’approccio multimodale e l’abbattimento al 3% dei casi destinati alla scialoadenectomia tradizionale, giustifica l’utilizzo in modo combinato di tali tecniche costose e time-consuming come parte integrante del moderno management della litiasi salivare. La radiologia interventistica, in particolar modo la riabilitazione duttale plastica mediante catetere a palloncino sotto controllo fluoroscopico, appare, nonostante l’impiego di radiazioni, la migliore opzione terapeutica nella gestione delle stenosi e dei kinkings duttali. L’endoscopia salivare operativa, da sola, rappresenta il trattamento di scelta per tutte le ostruzioni endoluminali mobili (microliti, mucous plugs o corpi estranei) e per il trattamento locale di patologie infiammatorie tra cui parotiti ricorrenti croniche o disordini salivari di origine autoimmune. In aggiunta a ciò, in caso di fallimento delle precedenti opzioni terapeutiche, indipendentemente dalla causa dell’ostruzione, l’infiltrazione di tossina botulinica nel parenchima salivare sotto controllo ecocolor Doppler dovrebbe essere considerata prima di optare per l’asportazione chirurgica della ghiandola salivare.
Figures


References
-
- Capaccio P, Minetti AM, Manzo R, Palazzo V, Ottaviani F. The role of the sialoendoscopy in the evaluation of obstructive salivary disease. Int J Maxillo Odontostomatol 2003;2:9-12.
-
- Brown AL, Shepherd D, Buckenham TM. Per oral balloon sialoplasty: results in the treatment of salivary duct stenosis. Cardiovasc Intervent Radiol 1997;20:337-42. - PubMed
-
- Escudier MP. The current status and possible future for lithotripsy of salivary calculi. In: Pregrel M, editor. Atlas of oral and maxillofacial surgery clinics of North America. Philadelphia, PA: Saunders; 1998. p. 117-32. - PubMed
-
- Marchal F, Kurt AM, Dulguerov P, Lehmann W. Retrograde theory in sialolithiasis formation. Arch Otolaryngol Head Neck Surg 2001;127:66-8. - PubMed
-
- Marchal F, Dulguerov P, Becker M, Barki G, Disant F, Lehmann W. Specificity for parotid sialendoscopy. Laryngoscope 2001;111:264-71. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical