

Are HIV positive patients resistant to statin therapy?
- PMID: 17958912
- PMCID: PMC2186312
- DOI: 10.1186/1476-511X-6-27
Are HIV positive patients resistant to statin therapy?
Abstract
Background: Patients with HIV are subject to development of HIV metabolic syndrome characterized by dyslipidemia, lipodystrophy and insulin resistance secondary to highly active antiretroviral therapy (HAART). Rosuvastatin is a highly potent HMG-CoA reductase inhibitor. Rosuvastatin is effective at lowering LDL and poses a low risk for drug-drug interaction as it does not share the same metabolic pathway as HAART drugs. This study sought to determine the efficacy of rosuvastatin on lipid parameters in HIV positive patients with HIV metabolic syndrome.
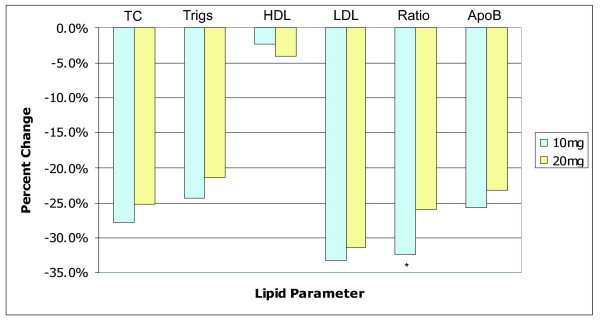
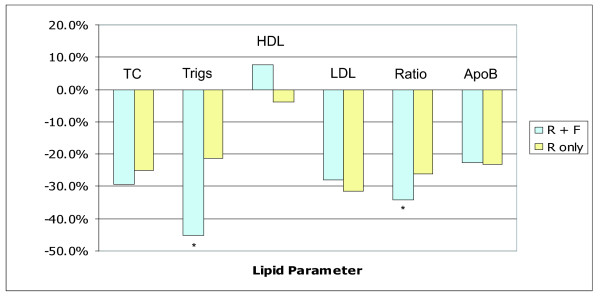
Results: Mean TC decreased from 6.54 to 4.89 mmol/L (25.0% reduction, p < 0.001). Mean LDL-C decreased from 3.39 to 2.24 mmol/L (30.8% reduction, p < 0.001). Mean HDL rose from 1.04 to 1.06 mmol/L (2.0% increase, p = ns). Mean triglycerides decreased from 5.26 to 3.68 mmol/L (30.1% reduction, p < 0.001). Secondary analysis examining the effectiveness of rosuvastatin monotherapy (n = 70) vs. rosuvastatin plus fenofibrate (n = 43) showed an improvement of 21.3% in TG and a decrease of 4.1% in HDL-C in the monotherapy group. The rosuvastatin plus fenofibrate showed a greater drop in triglycerides (45.3%, p < 0.001) and an increase in HDL of 7.6% (p = 0.08).
Conclusion: This study found that rosuvastatin is effective at improving potentially atherogenic lipid parameters in HIV-positive patients. The lipid changes we observed were of a smaller magnitude compared to non-HIV subjects. Our results are further supported by a small, pilot trial examining rosuvastatin effectiveness in HIV who reported similar median changes from baseline of -21.7% (TC), -22.4% (LDL-C), -30.1% (TG) with the exception of a 28.5% median increase in HDL. In light of the results revealed by this pilot study, clinicians may want to consider a possible resistance to statin therapy when treating patients with HIV metabolic syndrome.
Figures
References
-
- Periard D, Telenti A, Sudre P, Cheseaux JJ, Halfon P, Reymond MJ, Marcovina SM, Glauser MP, Nicod P, Darioli R, Mooser V. Atherogenic dyslipidemia in HIV-infected individuals treated with protease inhibitors. The Swiss HIV Cohort Study. Circulation. 1999;100:700–5. - PubMed
-
- Klein D, Hurley LB, Quesenberry CP, Jr, Sidney S. Do protease inhibitors increase the risk for coronary heart disease in patients with HIV-1 infection? J Acquir Immune Defic Syndr. 2002;30:471–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
