

Serologic evidence for reactivation of cryptococcosis in solid-organ transplant recipients
- PMID: 17959819
- PMCID: PMC2168388
- DOI: 10.1128/CVI.00242-07
Serologic evidence for reactivation of cryptococcosis in solid-organ transplant recipients
Abstract
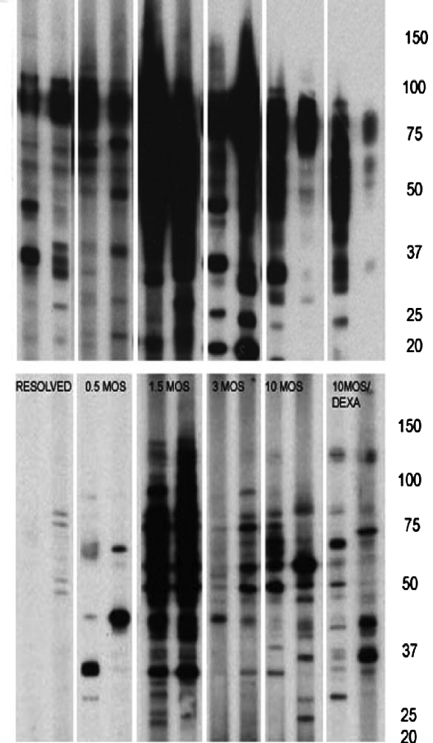
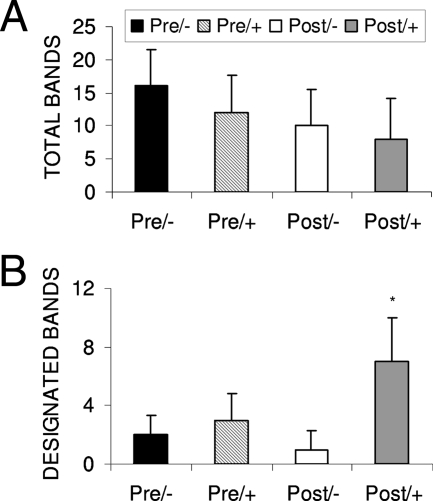
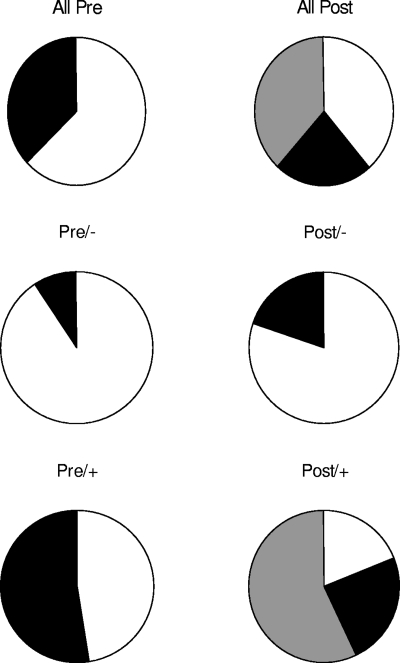
Cryptococcosis is a significant infection with a high mortality in solid-organ transplant recipients. Nonetheless, the pathogenesis of this disease is poorly understood. It has been hypothesized that cryptococcosis may result from either primary infection or reactivation of a latent infection. Sera were obtained from transplant recipients prior to transplantation and at the time they developed cryptococcosis. Control sera were obtained before and after transplant from patients who did not develop cryptococcosis. Sera were tested for antibodies against Cryptococcus neoformans by using an immunoblot assay. Antibody responses were also compared with those observed in sera from rats with experimental pulmonary cryptococcosis. In all, 52% of the transplant recipients who developed cryptococcosis exhibited serologic evidence of cryptococcal infection before transplantation. These patients developed cryptococcosis significantly earlier after transplant than patients without preexisting reactivity did (5.6 +/- 3.4 months compared to 40.6 +/- 63.8 months, respectively [P = 0.0011]). The results from our study suggest that a substantial proportion of transplant-associated cryptococcosis cases result from the reactivation of a latent infection. These findings also highlight the potential utility of serologic studies in identifying patients at risk for the development of cryptococcosis after transplantation.
Figures

References
-
- Davis, J., W. Y. Zeng, A. Glatman-Freedman, J.-A. Navoa Ng, M. R. Pagcatipunan, H. Lessin, A. Casadevall, and D. L. Goldman. 2007. Serologic evidence for regional differences in pediatric cryptococcal infection. Pediatr. Infect. Dis. J. 26:549-551. - PubMed
-
- Goldman, D. L., H. Khine, J. Abadi, D. J. Lindenberg, L.-A. Pirofski, R. Niang, et al. 2001. Serologic evidence for Cryptococcus neoformans infection in early childhood. Pediatrics 107:e66. - PubMed
-
- Goldman, D. L., S. C. Lee, A. J. Mednick, L. Montella, and A. Casadevall. 2000. Persistent Cryptococcus neoformans pulmonary infection in the rat is associated with intracellular parasitism, decreased inducible nitric oxide synthase expression, and altered antibody responsiveness to cryptococcal polysaccharide. Infect. Immun. 68:832-838. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
