

Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor
- PMID: 17962231
- PMCID: PMC2632426
- DOI: 10.1093/schbul/sbm114
Cognitive behavior therapy for schizophrenia: effect sizes, clinical models, and methodological rigor
Abstract
Background: Guidance in the United States and United Kingdom has included cognitive behavior therapy for psychosis (CBTp) as a preferred therapy. But recent advances have widened the CBTp targets to other symptoms and have different methods of provision, eg, in groups.
Aim: To explore the effect sizes of current CBTp trials including targeted and nontargeted symptoms, modes of action, and effect of methodological rigor.
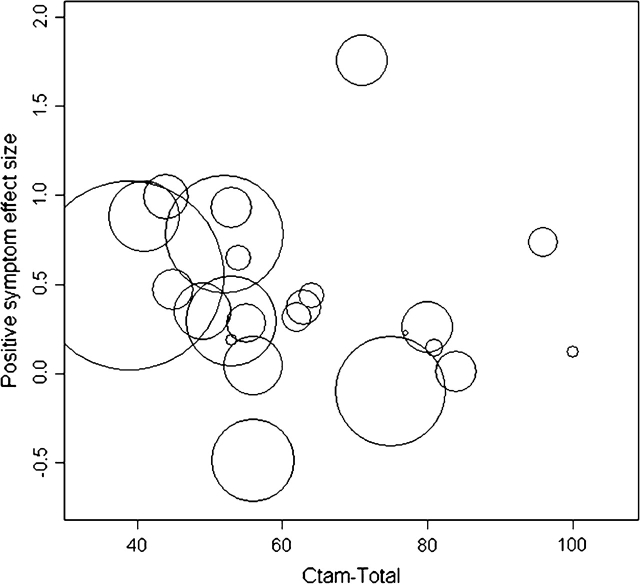
Method: Thirty-four CBTp trials with data in the public domain were used as source data for a meta-analysis and investigation of the effects of trial methodology using the Clinical Trial Assessment Measure (CTAM).
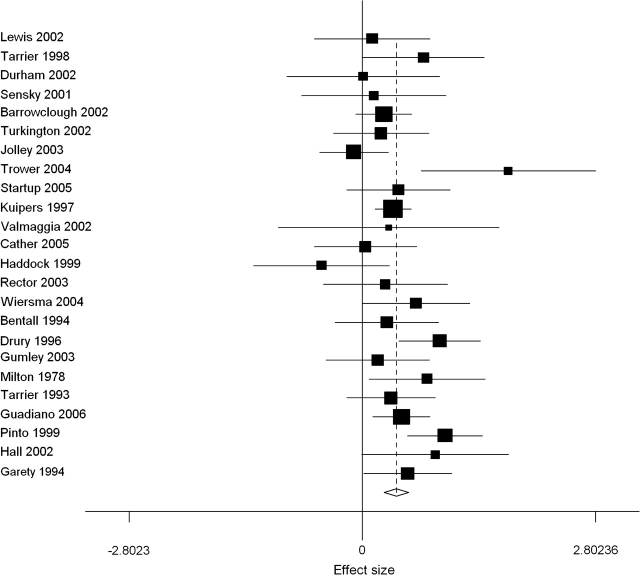
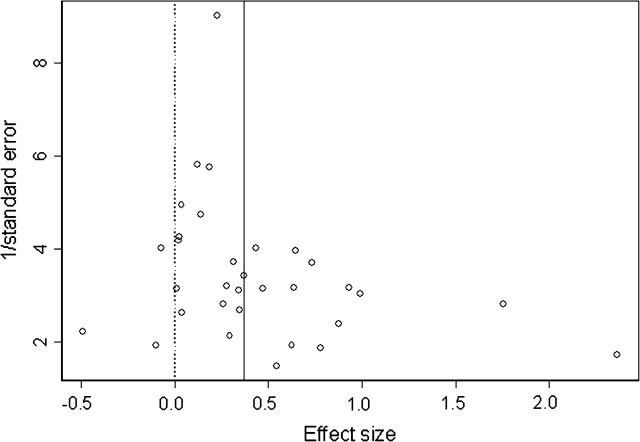
Results: There were overall beneficial effects for the target symptom (33 studies; effect size = 0.400 [95% confidence interval [CI] = 0.252, 0.548]) as well as significant effects for positive symptoms (32 studies), negative symptoms (23 studies), functioning (15 studies), mood (13 studies), and social anxiety (2 studies) with effects ranging from 0.35 to 0.44. However, there was no effect on hopelessness. Improvements in one domain were correlated with improvements in others. Trials in which raters were aware of group allocation had an inflated effect size of approximately 50%-100%. But rigorous CBTp studies showed benefit (estimated effect size = 0.223; 95% CI = 0.017, 0.428) although the lower end of the CI should be noted. Secondary outcomes (eg, negative symptoms) were also affected such that in the group of methodologically adequate studies the effect sizes were not significant.
Conclusions: As in other meta-analyses, CBTp had beneficial effect on positive symptoms. However, psychological treatment trials that make no attempt to mask the group allocation are likely to have inflated effect sizes. Evidence considered for psychological treatment guidance should take into account specific methodological detail.
Figures
References
-
- Beck AT. Successful out-patient psychotherapy of a chronic schizophrenic with a delusion based on borrowed guilt. Psychiatry. 1952;15:205–212. - PubMed
-
- Shapiro MB, Ravenette AT. A preliminary experiment on paranoid delusions. J Ment Sci. 1959;105:295–312. - PubMed
-
- Meichenbaum D, Cameron R. Training schizophrenics to talk to themselves: a means of developing attentional control. Behav Ther. 1973;4:515–534.
-
- Brown GW, Birley JLT, Wing JK. Influence of family life on course of schizophrenic disorders—replication. Br J Psychiatry. 1972;121:241–258. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
