

Diagnosis of the double aortic arch and its differentiation from the conotruncal malformations
- PMID: 17963340
- PMCID: PMC2628149
- DOI: 10.3349/ymj.2007.48.5.818
Diagnosis of the double aortic arch and its differentiation from the conotruncal malformations
Abstract
Purpose: The clinical and radiological characteristics of the double aortic arch (DAA) and its differentiation from conotruncal malformations (CTM) were reported in order to familiarize pediatric practitioners with these congenital heart diseases.
Materials and methods: From July 1994 to December 2006, a total of 6 patients (4 male and 2 female, aged 16 days to 6.5 years) with DAA were enrolled in this retrospective study. The study modalities included chart recordings, plain chest radiographs, barium esophagograms, echocardiograms, cardiac catheterization, cardiac angiograms, surgery, magnetic resonance imaging, and chromosome analysis. Patients with incomplete vascular rings or with right aortic arches and left ligamentum were excluded. In addition, the clinical and radiological profiles of 38 patients with CTM, including dextro-transposition of the great arteries (d-TGA) (n=28), hemitruncus arteriosus (HTA) (n=3), type I truncus arteriosus (TA) (n=4), and the aortopulmonary window (APW) (n=3), were comparatively reviewed.
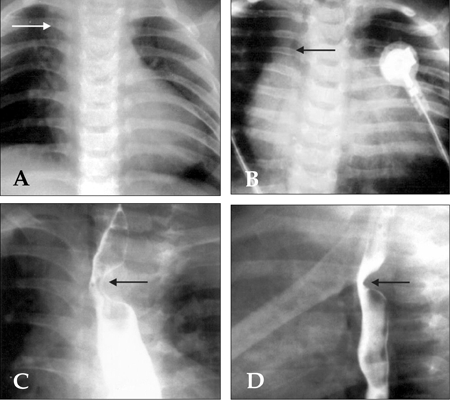
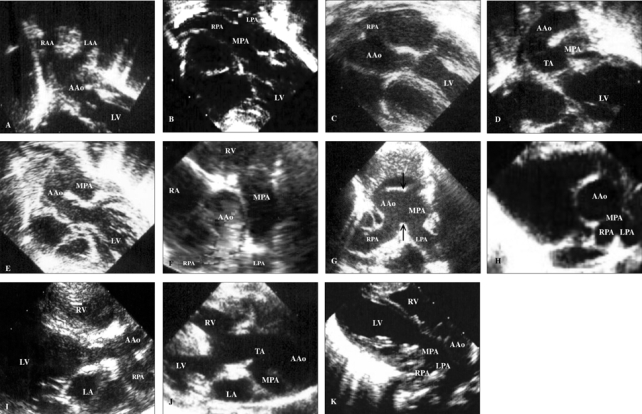
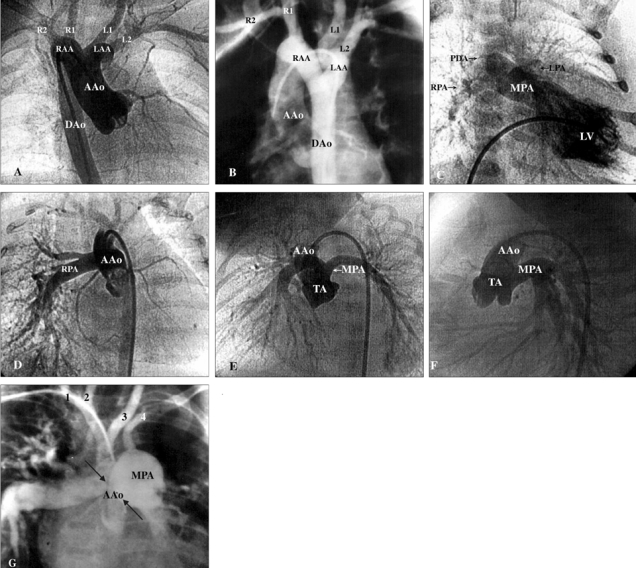
Results: All 6 patients with DAA presented with postprandial choking and respiratory distress that prompted their initial visit to the hospital. One of the 6 patients presented with congestive heart failure, and none with cyanosis. Esophagograms showed indentations in 5 patients with DAA. All patients with d-TGA presented with cyanosis and heart failure, while patients with HTA, type I TA, and APW manifested overt heart failure. Suprasternal and subcostal approaches of the echocardiography may offer diagnostic windows for DAA. As for CTM, parasternal and subcostal approaches could always determine the causality. Cardiac catheterization with angiography comprehensively delineated the pathology.
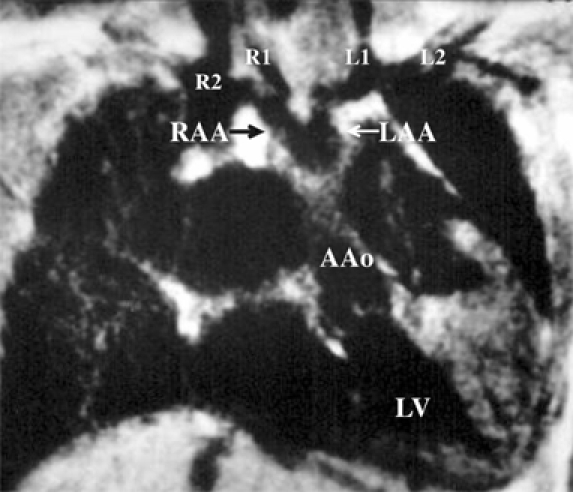
Conclusion: In case of postprandial choking and respiratory distress in neonates and infants, barium esophagograms can indicate the presence of DAA. Diagnosis of DAA and its differentiation from the CTM can be achieved by echocardiography, angiography, or magnetic resonance imaging.
Figures
Similar articles
-
Diagnosis and surgical repair of congenital double aortic arch in infants.J Cardiothorac Surg. 2019 Sep 9;14(1):160. doi: 10.1186/s13019-019-0976-x. J Cardiothorac Surg. 2019. PMID: 31500640 Free PMC article.
-
Persistent fifth aortic arch associated with 22q11.2 deletion syndrome.J Formos Med Assoc. 2006 Apr;105(4):284-9. doi: 10.1016/S0929-6646(09)60119-4. J Formos Med Assoc. 2006. PMID: 16618608
-
Truncus arteriosus with double aortic arch: A rare association.Turk J Pediatr. 2017;59(2):221-223. doi: 10.24953/turkjped.2017.02.020. Turk J Pediatr. 2017. PMID: 29276881
-
Vascular rings: 10-year review of imaging.Radiographics. 1991 Jul;11(4):637-46. doi: 10.1148/radiographics.11.4.1887119. Radiographics. 1991. PMID: 1887119 Review.
-
Anomalous subaortic left brachiocephalic vein in surgical cases and literature review.Clin Anat. 2010 Nov;23(8):950-5. doi: 10.1002/ca.21046. Clin Anat. 2010. PMID: 20830788 Review.
Cited by
-
Surgical treatment of double aortic arch malformation combined with descending aortic arch dissection in adults: a case series.J Cardiothorac Surg. 2023 May 9;18(1):174. doi: 10.1186/s13019-023-02244-y. J Cardiothorac Surg. 2023. PMID: 37161427 Free PMC article.
-
A case of balanced type double aortic arch diagnosed incidentally by transthoracic echocardiography in an asymptomatic adult patient.J Cardiovasc Ultrasound. 2011 Sep;19(3):163-6. doi: 10.4250/jcu.2011.19.3.163. Epub 2011 Sep 30. J Cardiovasc Ultrasound. 2011. PMID: 22073330 Free PMC article.
-
Balanced double aortic arch demonstrated by multimodality image and 7-year follow-up in a symptomatic elderly patient: A case report.Radiol Case Rep. 2022 Sep 19;17(11):4399-4402. doi: 10.1016/j.radcr.2022.08.051. eCollection 2022 Nov. Radiol Case Rep. 2022. PMID: 36188078 Free PMC article.
References
-
- Backer CL, Mavroudis C, Rigsby CK, Holinger LD. Trends in vascular ring surgery. J Thorac Cardiovasc Surg. 2005;129:1339–1347. - PubMed
-
- Alsenaidi K, Gurofsky R, Karamlou T, Williams WG, McCrindle BW. Management and outcomes of double aortic arch in 81 patients. Pediatrics. 2006;118:e1336–e1341. - PubMed
-
- Backer CL, Mavroudis C. Congenital Heart Surgery Nomenclature and Database Project: vascular rings, tracheal stenosis, pectus excavatum. Ann Thorac Surg. 2000;69(4 Suppl):S308–S318. - PubMed
-
- Blumenthal S, Ravitch MM. Seminar on aortic vascular rings and other anomalies of the aortic arch. Pediatrics. 1957;20:896–906. - PubMed
-
- Griswold HE, Young MD. Double aortic arch; Report of two cases and review of the literature. Pediatrics. 1949;4:751–768. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
