

A web-based laboratory information system to improve quality of care of tuberculosis patients in Peru: functional requirements, implementation and usage statistics
- PMID: 17963522
- PMCID: PMC2198908
- DOI: 10.1186/1472-6947-7-33
A web-based laboratory information system to improve quality of care of tuberculosis patients in Peru: functional requirements, implementation and usage statistics
Abstract
Background: Multi-drug resistant tuberculosis patients in resource-poor settings experience large delays in starting appropriate treatment and may not be monitored appropriately due to an overburdened laboratory system, delays in communication of results, and missing or error-prone laboratory data. The objective of this paper is to describe an electronic laboratory information system implemented to alleviate these problems and its expanding use by the Peruvian public sector, as well as examine the broader issues of implementing such systems in resource-poor settings.
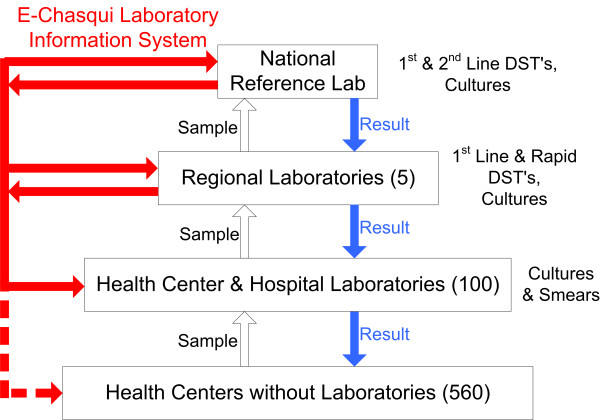
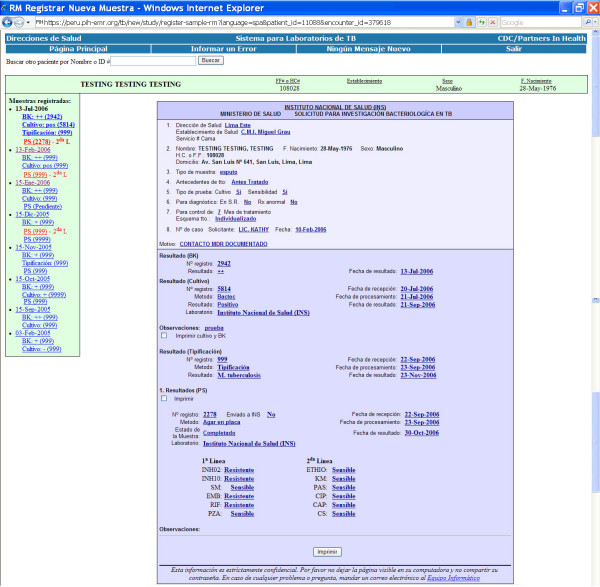
Methods: A web-based laboratory information system "e-Chasqui" has been designed and implemented in Peru to improve the timeliness and quality of laboratory data. It was deployed in the national TB laboratory, two regional laboratories and twelve pilot health centres. Using needs assessment and workflow analysis tools, e-Chasqui was designed to provide for improved patient care, increased quality control, and more efficient laboratory monitoring and reporting.
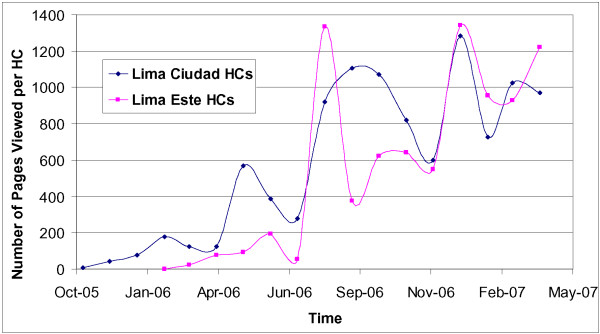
Results: Since its full implementation in March 2006, 29,944 smear microscopy, 31,797 culture and 7,675 drug susceptibility test results have been entered. Over 99% of these results have been viewed online by the health centres. High user satisfaction and heavy use have led to the expansion of e-Chasqui to additional institutions. In total, e-Chasqui will serve a network of institutions providing medical care for over 3.1 million people. The cost to maintain this system is approximately US$0.53 per sample or 1% of the National Peruvian TB program's 2006 budget.
Conclusion: Electronic laboratory information systems have a large potential to improve patient care and public health monitoring in resource-poor settings. Some of the challenges faced in these settings, such as lack of trained personnel, limited transportation, and large coverage areas, are obstacles that a well-designed system can overcome. e-Chasqui has the potential to provide a national TB laboratory network in Peru. Furthermore, the core functionality of e-Chasqui as been implemented in the open source medical record system OpenMRS http://www.openmrs.org for other countries to use.
Figures
References
-
- Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, Zeller K, Andrews J, Friedland G. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006;368:1575–1580. doi: 10.1016/S0140-6736(06)69573-1. - DOI - PubMed
-
- Hurtado R. Personal Communication. 2006.
-
- Park MM, Davis AL, Schluger NW, Cohen H, Rom WN. Outcome of MDR-TB patients, 1983–1993. Prolonged survival with appropriate therapy. Am J Respir Crit Care Med. 1996;153:317–324. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
