

Phase I pharmacokinetic and pharmacodynamic study of temozolomide in pediatric patients with refractory or recurrent leukemia: a Children's Oncology Group Study
- PMID: 17971589
- PMCID: PMC6684202
- DOI: 10.1200/JCO.2007.12.0667
Phase I pharmacokinetic and pharmacodynamic study of temozolomide in pediatric patients with refractory or recurrent leukemia: a Children's Oncology Group Study
Abstract
Purpose: To determine the tolerability, pharmacokinetics, and mechanisms of temozolomide resistance in children with relapsed or refractory leukemia.
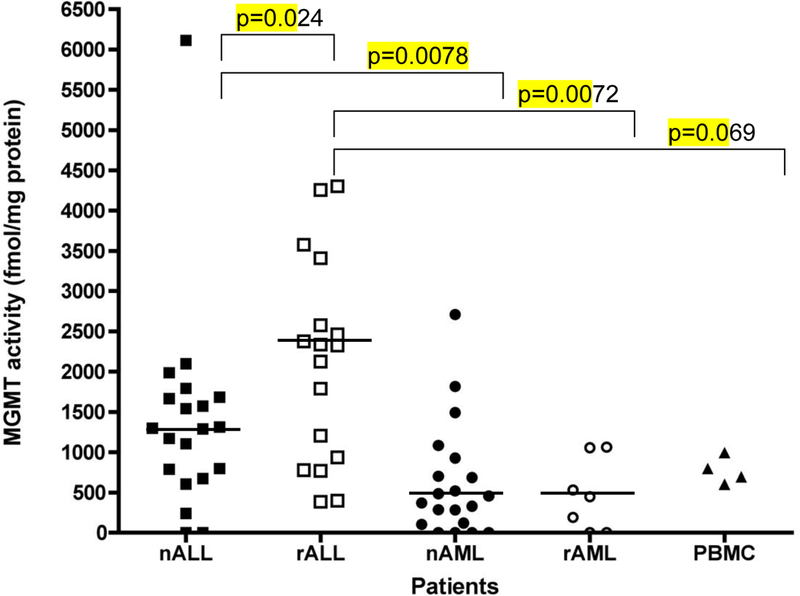
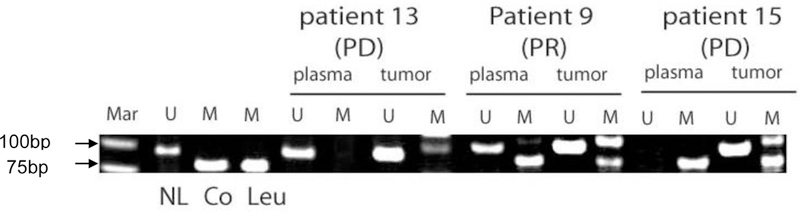
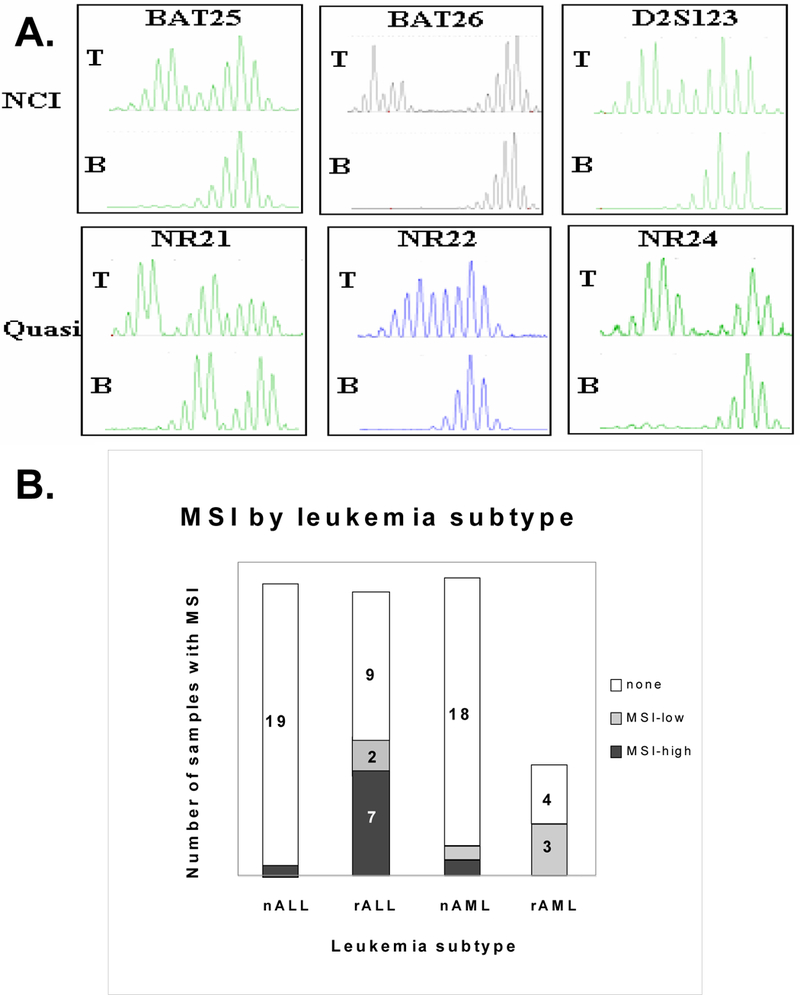
Patients and methods: Cohorts of three to six patients received 200 or 260 mg/m2/d of temozolomide by mouth daily for 5 days every 28 days. Toxicities, clinical response, and pharmacokinetics were evaluated. Pretreatment leukemia cell O6-methylguanine-DNA methyltransferase (MGMT) activity, tumor and plasma MGMT promoter methylation, and microsatellite instability (MSI) were examined in 14 of 16 study patients and in tissue bank samples from children with acute leukemia not treated with temozolomide (MGMT, n = 67; MSI, n = 65).
Results: Sixteen patients (nine female, seven male; acute lymphoblastic leukemia [ALL], n = 8; acute myeloid leukemia [AML], n = 8), median age 11 years (range, 1 to 19 years), received either 200 mg/m2/d (nine enrolled, three assessable for toxicity) or 260 mg/m2/d (seven enrolled, three assessable for toxicity) of temozolomide. Temozolomide was well tolerated and no dose-limiting toxicities occurred. The mean clearance of temozolomide was 107 mL/min/m2, with a volume of distribution of 20 L/m2 and half-life of 109 minutes. MGMT activity in leukemia cells was quite variable and was highest in patients with relapsed ALL. Only one patient had MSI. Two patients had a partial response. Both of these patients had no detectable MGMT activity; both also had methylated MGMT promoters and were MSI stable.
Conclusion: Temozolomide was well tolerated at doses as high as 260 mg/m2/d for 5 days in children with relapsed or refractory leukemia. Increased MGMT activity may account for the temozolomide resistance in children with relapsed leukemia. Leukemia cell MGMT activity was higher in pediatric ALL than AML (P < .0001).
Figures
Similar articles
-
Promoter methylation and expression analysis of MGMT in advanced pediatric brain tumors.Oncol Rep. 2009 Oct;22(4):773-9. doi: 10.3892/or_00000499. Oncol Rep. 2009. PMID: 19724855 Clinical Trial.
-
Salvage treatment with temozolomide in refractory or relapsed primary central nervous system lymphoma and assessment of the MGMT status.J Neurooncol. 2012 Jan;106(1):155-60. doi: 10.1007/s11060-011-0652-z. Epub 2011 Jul 1. J Neurooncol. 2012. PMID: 21720808
-
A pediatric phase 1 trial of vorinostat and temozolomide in relapsed or refractory primary brain or spinal cord tumors: a Children's Oncology Group phase 1 consortium study.Pediatr Blood Cancer. 2013 Sep;60(9):1452-7. doi: 10.1002/pbc.24541. Epub 2013 Mar 28. Pediatr Blood Cancer. 2013. PMID: 23554030 Free PMC article. Clinical Trial.
-
MGMT Expression Contributes to Temozolomide Resistance in H3K27M-Mutant Diffuse Midline Gliomas and MGMT Silencing to Temozolomide Sensitivity in IDH-Mutant Gliomas.Neurol Med Chir (Tokyo). 2018 Jul 15;58(7):290-295. doi: 10.2176/nmc.ra.2018-0044. Epub 2018 May 31. Neurol Med Chir (Tokyo). 2018. PMID: 29848907 Free PMC article. Review.
-
Regulation of expression of O6-methylguanine-DNA methyltransferase and the treatment of glioblastoma (Review).Int J Oncol. 2015 Aug;47(2):417-28. doi: 10.3892/ijo.2015.3026. Epub 2015 May 29. Int J Oncol. 2015. PMID: 26035292 Free PMC article. Review.
Cited by
-
NEO212, a Perillyl Alcohol-Temozolomide Conjugate, Triggers Macrophage Differentiation of Acute Myeloid Leukemia Cells and Blocks Their Tumorigenicity.Cancers (Basel). 2022 Dec 9;14(24):6065. doi: 10.3390/cancers14246065. Cancers (Basel). 2022. PMID: 36551551 Free PMC article.
-
Phase 1/2 trial of talazoparib in combination with temozolomide in children and adolescents with refractory/recurrent solid tumors including Ewing sarcoma: A Children's Oncology Group Phase 1 Consortium study (ADVL1411).Pediatr Blood Cancer. 2020 Feb;67(2):e28073. doi: 10.1002/pbc.28073. Epub 2019 Nov 14. Pediatr Blood Cancer. 2020. PMID: 31724813 Free PMC article. Clinical Trial.
-
A Multicenter Randomized Bioequivalence Study of a Novel Ready-to-Use Temozolomide Oral Suspension vs. Temozolomide Capsules.Pharmaceutics. 2023 Nov 24;15(12):2664. doi: 10.3390/pharmaceutics15122664. Pharmaceutics. 2023. PMID: 38140005 Free PMC article.
-
Poly(ADP-ribose) polymerase inhibitor ABT-888 potentiates the cytotoxic activity of temozolomide in leukemia cells: influence of mismatch repair status and O6-methylguanine-DNA methyltransferase activity.Mol Cancer Ther. 2009 Aug;8(8):2232-42. doi: 10.1158/1535-7163.MCT-09-0142. Epub 2009 Aug 11. Mol Cancer Ther. 2009. PMID: 19671751 Free PMC article.
-
Pharmacokinetics of temozolomide administered in combination with O6-benzylguanine in children and adolescents with refractory solid tumors.Cancer Chemother Pharmacol. 2009 Dec;65(1):137-42. doi: 10.1007/s00280-009-1015-8. Epub 2009 May 9. Cancer Chemother Pharmacol. 2009. PMID: 19430790 Free PMC article. Clinical Trial.
References
-
- Friedman HS, Kerby T, and Calvert H Temozolomide and treatment of malignant glioma. Clin.Cancer Res, 6: 2585–2597, 2000. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, Weller M, Fisher B, Taphoorn MJ, Belanger K, Brandes AA, Marosi C, Bogdahn U, Curschmann J, Janzer RC, Ludwin SK, Gorlia T, Allgeier A, Lacombe D, Cairncross JG, Eisenhauer E, and Mirimanoff RO Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N.Engl.J Med, 352: 987–996, 2005. - PubMed
-
- Tentori L, Graziani G, Gilberti S, Lacal PM, Bonmassar E, and D’Atri S Triazene compounds induce apoptosis in O6-alkylguanine-DNA alkyltransferase deficient leukemia cell lines. Leukemia, 9: 1888–1895, 1995. - PubMed
-
- Messinger Y, Reaman GH, Ek O, and Uckun FM Evaluation of temozolomide in a SCID mouse model of human B-cell precursor leukemia. Leuk Lymphoma, 33: 289–293, 1999. - PubMed
-
- Seiter K, Liu D, Loughran T, Siddiqui A, Baskind P, and Ahmed T Phase I study of temozolomide in relapsed/refractory acute leukemia. J Clin Oncol, 20: 3249–3253, 2002. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
