

Autologous platelet gel and platelet-poor plasma reduce pain with total shoulder arthroplasty
- PMID: 17972452
- PMCID: PMC4680728
Autologous platelet gel and platelet-poor plasma reduce pain with total shoulder arthroplasty
Abstract
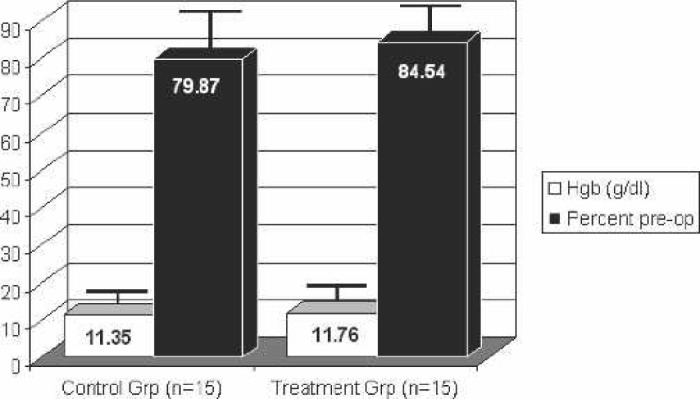
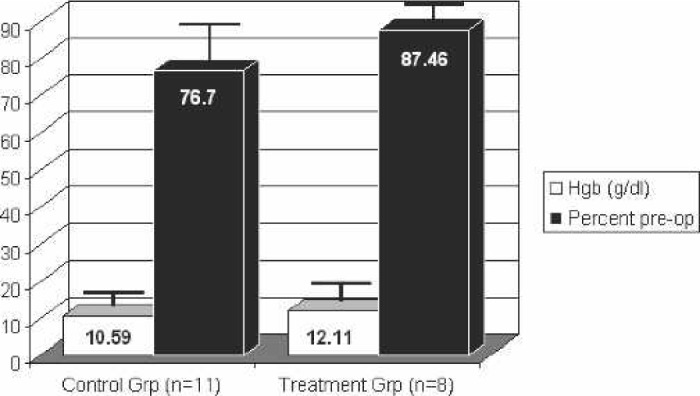
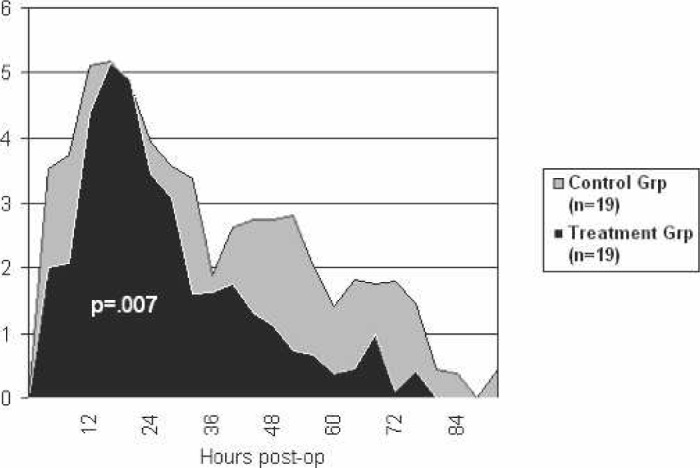
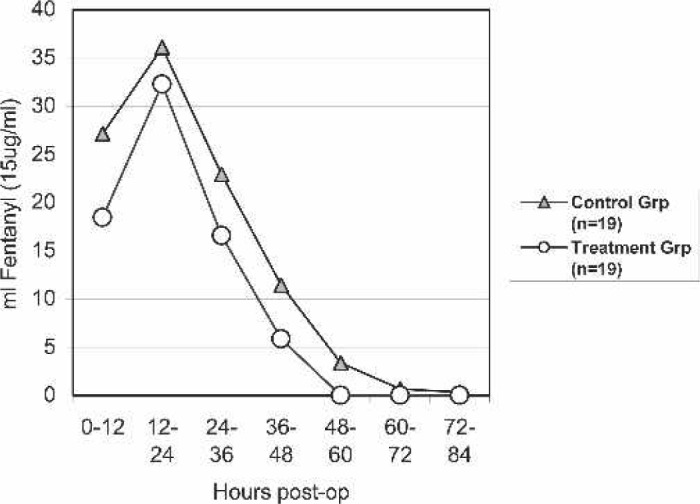
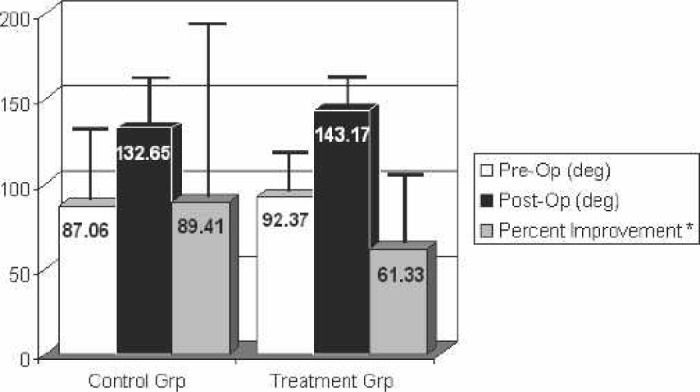
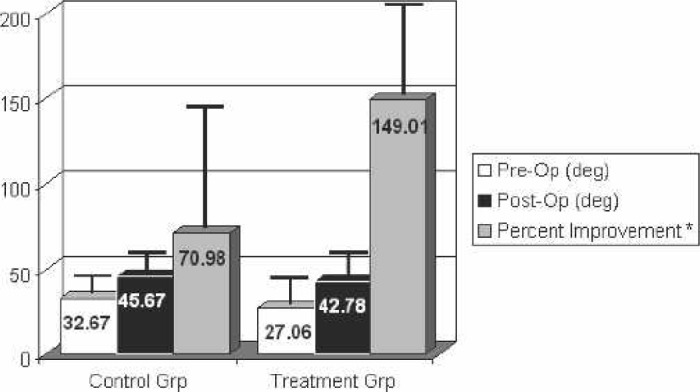
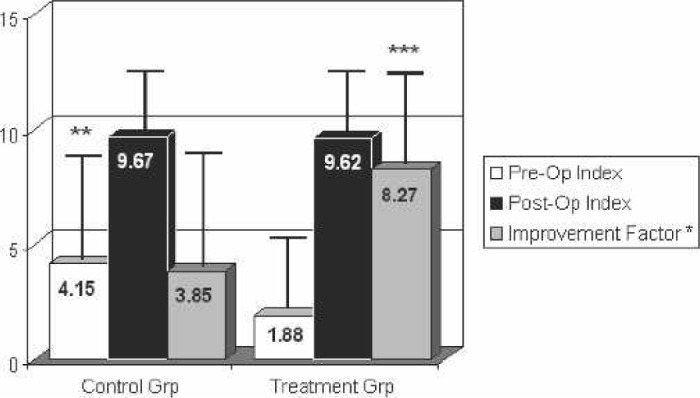
The recovery of patients undergoing total shoulder arthroplasty (TSA) can be adversely affected by a number of complications. Autologous platelet gel (APG), produced by activating platelet-rich plasma (PRP), has been shown to improve hemostasis and wound healing and reduce infections in some surgical procedures. Activated platelet-poor plasma (PPP) has also been used as a hemostatic agent. This study examines the effects of APG and PPP treatment on TSA patients postoperatively. After Institutional Review Board (IRB) approval, 40 patients undergoing TSA at our institution were prospectively enrolled in our study. They were randomized into either a control (n = 20) or study (n = 20) group, with the study group receiving APG and PPP treatment. Preoperative demographic data, pre- and postoperative laboratory data, pain scores, pain medication, complications, pre- and postoperative range of motion measurements, and postoperative lengths of stay were recorded for each group. The preoperative internal rotation index was significantly higher in the control group compared with treatment patients (4.64 +/- 4.46 vs. 1.88 +/- 2.44, p < .05). The percent hemoglobin retained postoperatively was higher in the treatment group at 24 (84.54 +/- 5.32 vs. 79.87 +/- 8.73) and 72 hours (87.46 +/- 16.03 vs. 76.70 vs. 5.96), but neither difference reached statistical significance. The treatment group had significantly lower pain scores (p = .007) and total fentanyl requirements (p < .05) compared with control patients. The internal rotation index improvement factor (postoperative internal rotation index/preoperative internal rotation index) was significantly higher in the treatment group vs. the control group (p < .05). Although it did not reach statistical significance, the treatment group was discharged almost 9 hours earlier than the control group (64.44 +/- 15.23 vs. 73.39 +/- 15.37). APG and PPP treatment decreased pain and provided a greater increase in internal rotation measurements postoperatively.
Conflict of interest statement
The senior editor has stated that authors have reported no material, financial or other relationship with any healthcare-related business or other entity whose products or services are discussed in this paper.
Figures
References
-
- Craig EV.. Master Techniques in Orthopaedic Surgery: The Shoulder. 2nd ed. Philadelphia: Lippincott, Williams & Wilkins; 2004.
-
- Schilling McCann JA.. Professional Guide to Pathophysiology. Philadelphia: Lippincott, Williams & Wilkins; 2003;409–12.
-
- Matsen FA III, Rockwood CA Jr, Wirth MA, et al. Glenohumeral arthritis and its management. In: Rockwood CA Jr, Matsen FA III, Wirth MA, et al. eds. The Shoulder. Philadelphia: Saunders; 2004; 879–1008.
-
- Cofield RH, Chang W, Sperling JW.. Complications of shoulder arthroplasty. In: Iannotti JR, Williams GR, eds. Disorders of the Shoulder: Diagnosis and Management. Philadelphia: Lippincott, Williams & Wilkins; 1999; 571–93.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials