

Preliminary experience with onyx embolization for the treatment of intracranial dural arteriovenous fistulas
- PMID: 17974618
- PMCID: PMC8119122
- DOI: 10.3174/ajnr.A0768
Preliminary experience with onyx embolization for the treatment of intracranial dural arteriovenous fistulas
Abstract
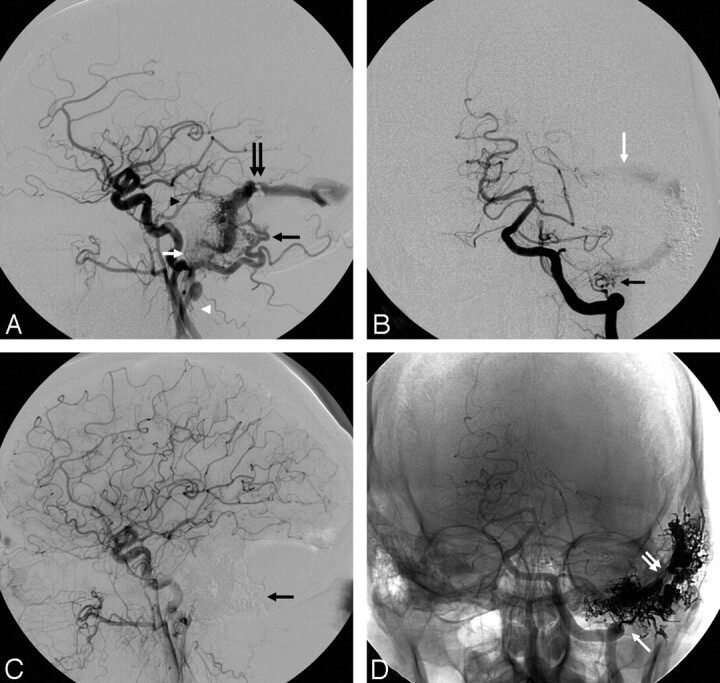
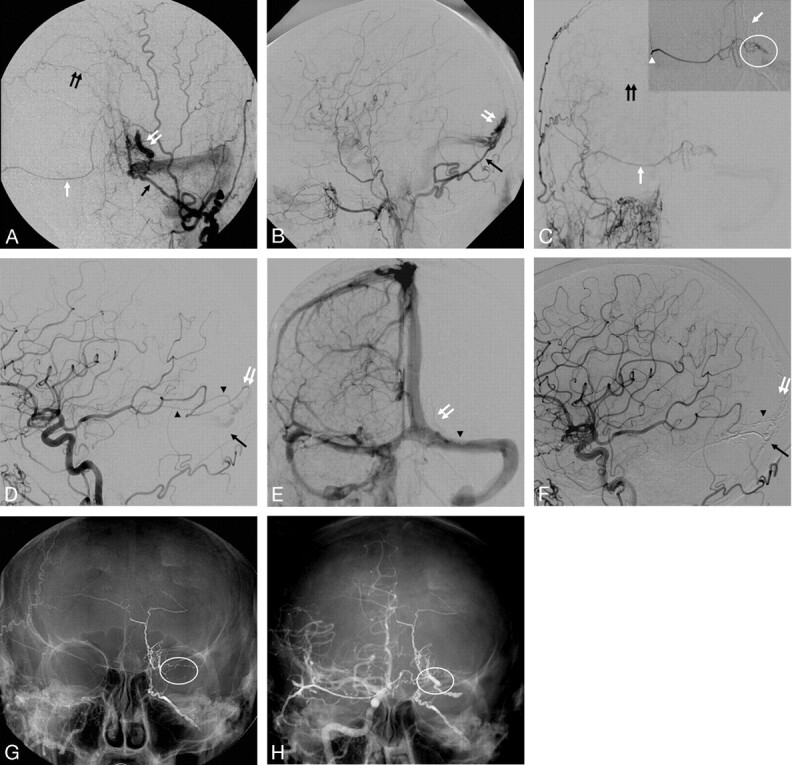
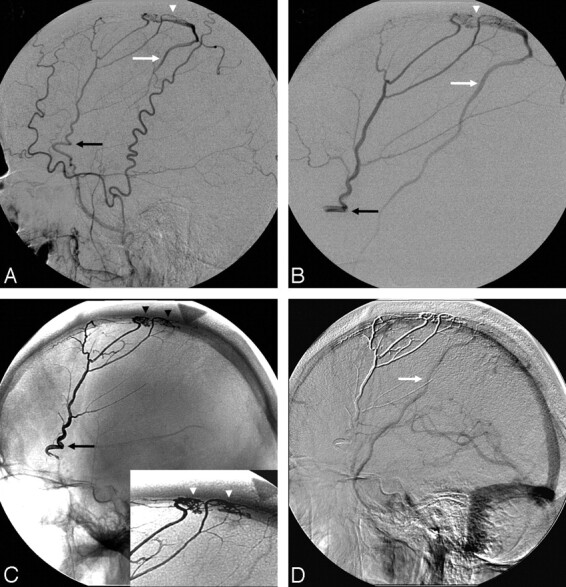
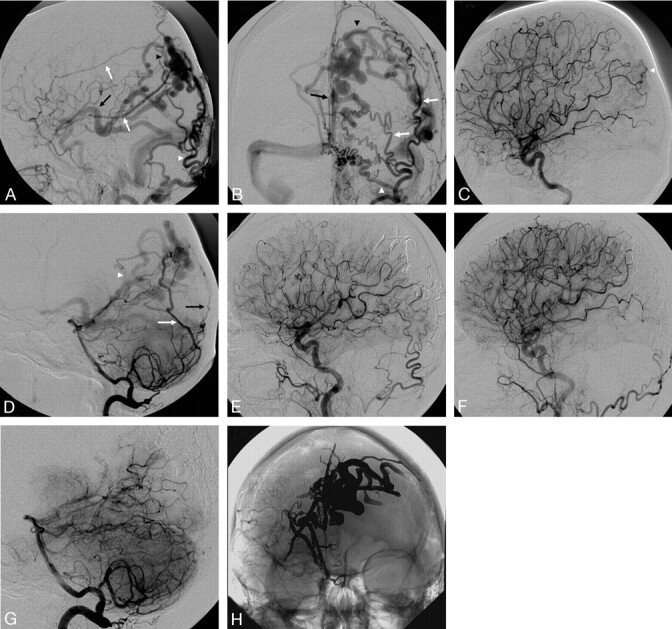
Background and purpose: Onyx was recently approved for the treatment of pial arteriovenous malformations, but its use to treat dural arteriovenous fistulas (DAVFs) is not yet well established. We now report on the treatment of intracranial DAVFs using this nonadhesive liquid embolic agent.
Materials and methods: We performed a retrospective analysis of 12 consecutive patients with intracranial DAVFs who were treated with Onyx as the single treatment technique at our institution between March 2006 and February 2007.
Results: A total of 17 procedures were performed in 12 patients. In all of the cases, transarterial microcatheterization was performed, and Onyx-18 or a combination of Onyx-18/Onyx-34 was used. Eight patients were men. The mean age was 56 +/- 12 years. Nine patients were symptomatic. There was an average of 5 feeders per DAVF (range, 1-9). Cortical venous reflux was present in all of the cases except for 1 of the symptomatic patients. Complete resolution of the DAVF on immediate posttreatment angiography was achieved in 10 patients. The remaining 2 patients had only minimal residual shunting postembolization, 1 of whom appeared cured on a follow-up angiogram 8 weeks later. The other patient has not yet had angiographic follow-up. Follow-up angiography (mean, 4.4 months) is currently available in 9 patients. There was 1 angiographic recurrence (asymptomatic), which was subsequently re-embolized with complete occlusion of the fistula and its draining vein. There was no significant morbidity or mortality.
Conclusion: In our experience, the endovascular treatment of intracranial DAVFs with Onyx is feasible, safe, and highly effective with a small recurrence rate in the short-term follow-up.
Figures
References
-
- Newton TH, Cronqvist S. Involvement of dural arteries in intracranial arteriovenous malformations. Radiology 1969;93:1071–78 - PubMed
-
- Sarma D, ter Brugge K. Management of intracranial dural arteriovenous shunts in adults. Eur J Radiol 2003;46:206–20 - PubMed
-
- van Dijk JM, terBrugge KG, Willinsky RA, et al. Clinical course of cranial dural arteriovenous fistulas with long-term persistent cortical venous reflux. Stroke 2002;33:1233–36 - PubMed
-
- Duffau H, Lopes M, Janosevic V, et al. Early rebleeding from intracranial dural arteriovenous fistulas: report of 20 cases and review of the literature. J Neurosurg 1999;90:78–84 - PubMed
-
- Kiyosue H, Hori Y, Okahara M, et al. Treatment of intracranial dural arteriovenous fistulas: current strategies based on location and hemodynamics, and alternative techniques of transcatheter embolization. Radiographics 2004;24:1637–53 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources