

Effects of corticosteroid on Henoch-Schönlein purpura: a systematic review
- PMID: 17974746
- PMCID: PMC3525094
- DOI: 10.1542/peds.2007-0667
Effects of corticosteroid on Henoch-Schönlein purpura: a systematic review
Abstract
Objective: No consensus exists among general pediatricians or pediatric rheumatologists regarding whether corticosteroid therapy ameliorates the acute manifestations of Henoch-Schönlein purpura or mitigates renal injury. Therefore, we sought to synthesize the reported experimental and observational data regarding corticosteroid use.
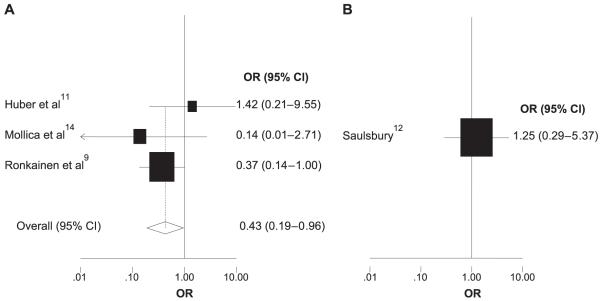
Methods: We performed a meta-analysis based on a comprehensive review of the literature in the Medline database (1956 to January 2007) and the Cochrane Controlled Trials Register. On the basis of reported outcomes among patients with Henoch-Schönlein purpura who were treated at diagnosis with corticosteroids compared with patients treated with supportive care only, we calculated odds ratios for the resolution of abdominal pain, the need for surgical intervention secondary to severe pain or intussusception, the likelihood of Henoch-Schönlein purpura recurrence, and the development of transient or persistent renal disease.
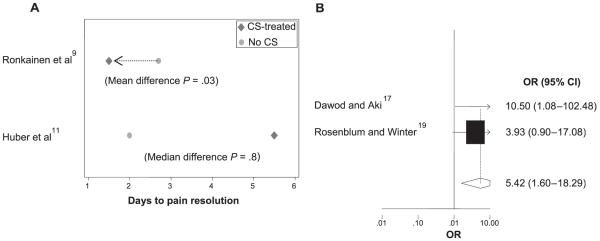
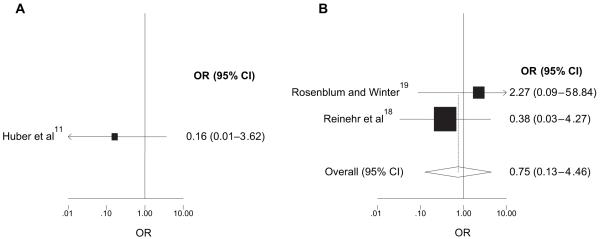
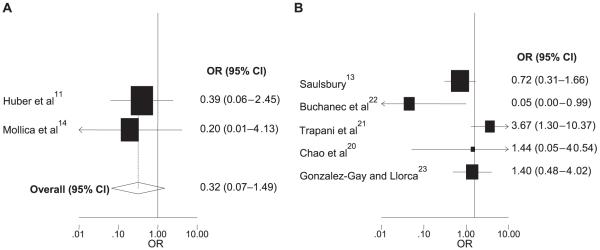
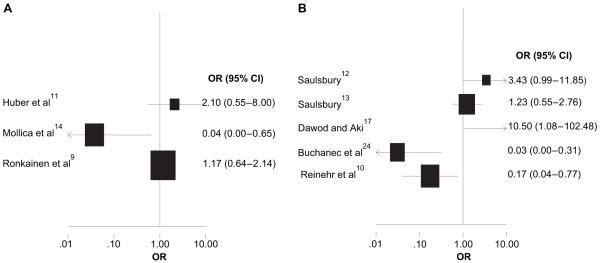
Results: Of 201 articles retrieved from the initial literature search, 15 were eligible for inclusion. Corticosteroid treatment did not reduce the median time to resolution of abdominal pain but did significantly reduce the mean resolution time and increased the odds of resolution within 24 hours. Early corticosteroid treatment significantly reduced the odds of developing persistent renal disease. In addition, although the results were not statistically significant, the prospective data suggest reduced odds of both surgical intervention and recurrence.
Conclusions: Corticosteroids, given early in the course of illness, seem to produce consistent benefits for several major clinically relevant Henoch-Schönlein purpura outcomes.
Figures
Comment in
-
Corticosteroid therapy for Henoch Schönlein purpura.Pediatrics. 2008 Apr;121(4):870-1; author reply 871-2. doi: 10.1542/peds.2008-0138. Pediatrics. 2008. PMID: 18381559 No abstract available.
References
-
- Bowyer S, Roettcher P, Pediatric rheumatology, Pediatric Rheumatology Database Research Group clinic populations in the United States: results of a 3 year survey. J Rheumatol. 1996;23:1968–1974. - PubMed
-
- Rostoker G. Schönlein-Henoch purpura in children and adults: diagnosis, pathophysiology and management. BioDrugs. 2001;15:99–138. - PubMed
-
- Kobayashi O, Wada H, Okawa K, Takeyama I. Schönlein-Henoch’s syndrome in children. Contrib Nephrol. 1975;4:48–71. - PubMed
-
- Calviño MC, Llorca J, García-Porrúa C, Fernández-Iglesias JL, Rodriguez-Ledo P, González-Gay MA. Henoch-Schönlein purpura in children from northwestern Spain: a 20-year epidemiologic and clinical study. Medicine (Baltimore) 2001;80:279–290. - PubMed
-
- Levy M, Broyer M, Arsan A, Levy-Bentolila D, Habib R. Anaphylactoid purpura nephritis in childhood: natural history and immunopathology. Adv Nephrol Necker Hosp. 1976;6:183–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
