

Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study
- PMID: 17977819
- PMCID: PMC2078636
- DOI: 10.1136/bmj.39363.706956.55
Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study
Abstract
Objective: To assess the risks and benefits associated with caesarean delivery compared with vaginal delivery.
Design: Prospective cohort study within the 2005 WHO global survey on maternal and perinatal health.
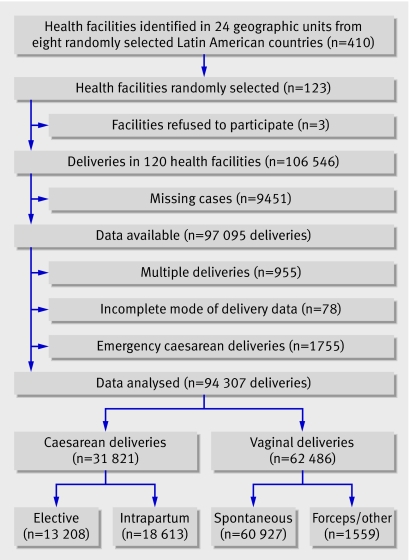
Setting: 410 health facilities in 24 areas in eight randomly selected Latin American countries; 123 were randomly selected and 120 participated and provided data
Participants: 106,546 deliveries reported during the three month study period, with data available for 97,095 (91% coverage).
Main outcome measures: Maternal, fetal, and neonatal morbidity and mortality associated with intrapartum or elective caesarean delivery, adjusted for clinical, demographic, pregnancy, and institutional characteristics.
Results: Women undergoing caesarean delivery had an increased risk of severe maternal morbidity compared with women undergoing vaginal delivery (odds ratio 2.0 (95% confidence interval 1.6 to 2.5) for intrapartum caesarean and 2.3 (1.7 to 3.1) for elective caesarean). The risk of antibiotic treatment after delivery for women having either type of caesarean was five times that of women having vaginal deliveries. With cephalic presentation, there was a trend towards a reduced odds ratio for fetal death with elective caesarean, after adjustment for possible confounding variables and gestational age (0.7, 0.4 to 1.0). With breech presentation, caesarean delivery had a large protective effect for fetal death. With cephalic presentation, however, independent of possible confounding variables and gestational age, intrapartum and elective caesarean increased the risk for a stay of seven or more days in neonatal intensive care (2.1 (1.8 to 2.6) and 1.9 (1.6 to 2.3), respectively) and the risk of neonatal mortality up to hospital discharge (1.7 (1.3 to 2.2) and 1.9 (1.5 to 2.6), respectively), which remained higher even after exclusion of all caesarean deliveries for fetal distress. Such increased risk was not seen for breech presentation. Lack of labour was a risk factor for a stay of seven or more days in neonatal intensive care and neonatal mortality up to hospital discharge for babies delivered by elective caesarean delivery, but rupturing of membranes may be protective.
Conclusions: Caesarean delivery independently reduces overall risk in breech presentations and risk of intrapartum fetal death in cephalic presentations but increases the risk of severe maternal and neonatal morbidity and mortality in cephalic presentations.
Conflict of interest statement
Competing interests: None declared.
Comment in
-
Maternal and neonatal effects of caesarean section.BMJ. 2007 Nov 17;335(7628):1003-4. doi: 10.1136/bmj.39372.587650.80. Epub 2007 Oct 30. BMJ. 2007. PMID: 17977818 Free PMC article.
-
Caesarean section: Points raised in responses.BMJ. 2007 Dec 15;335(7632):1226. doi: 10.1136/bmj.39423.481285.BE. BMJ. 2007. PMID: 18079524 Free PMC article. No abstract available.
-
Risks and benefits associated with caesarean delivery.Midwives. 2008 Feb-Mar;11(1):18. Midwives. 2008. PMID: 24902278 No abstract available.
References
-
- Hamilton B, Minino A, Martin J, Kochanek K, Strobino D, Guyer B. Annual summary of vital statistics: 2005. Pediatrics 2007;119:345-60. - PubMed
-
- Althabe F, Belizan JM, Villar J, Alexander S, Bergel E, Ramos S, et al. Mandatory second opinion to reduce rates of unnecessary caesarean sections in Latin America: a cluster randomised controlled trial. Lancet 2004;363:1934-40. - PubMed
-
- Minkoff H, Powderly K, Chervenak F, McCullough L. Ethical dimensions of elective primary cesarean delivery. Obstet Gynecol 2004;103:387-92. - PubMed
-
- Kalish R, McCullough L, Gupta M, Thaler H, Chervenak F. Intrapartum elective cesarean delivery: a previously unrecognized clinical entity. Obstet Gynecol 2004;103:1137-41. - PubMed
-
- Villar J, Valladares E, Wojdyla D, Zabaleta N, Carroli G, Velazco A, et al. Caesarean delivery rates and pregnancy outcomes: the 2005 WHO global survey on maternal and perinatal health in Latin America. Lancet 2006;367:1819-29. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical