

Review
doi: 10.1523/JNEUROSCI.3565-07.2007.
Stress and disease: is being female a predisposing factor?
Affiliations
- PMID: 17978023
- PMCID: PMC6673348
- DOI: 10.1523/JNEUROSCI.3565-07.2007
Item in Clipboard
Review
Stress and disease: is being female a predisposing factor?
J Neurosci.
.
No abstract available
Figures
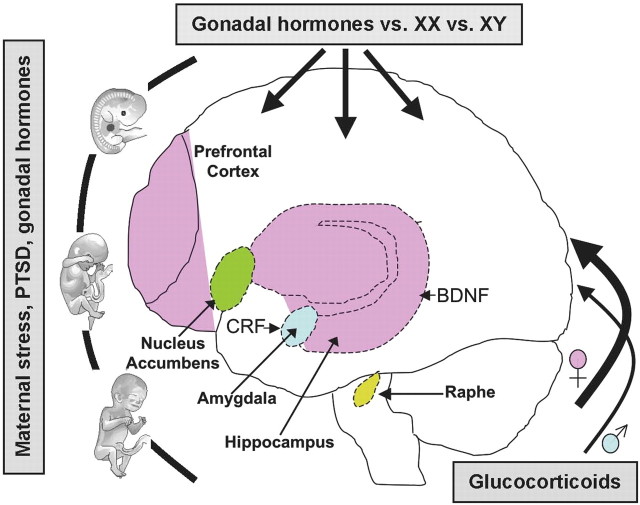
Schematic representing potential brain regions and genes involved in stress-related disease that are implicated in putative sex differences. These brain areas are highly interconnected with one another with numerous efferent and afferent projections involved in emotion, stress reactivity, and reward. Importantly, studies implicate sex differences in structure and/or function as modeled by prenatal or postnatal or adult stress experience. Uterine environment, including stress and gonadal hormones, can influence life susceptibility toward disease. Gonadal hormones (e.g., testosterone, estradiol, and progesterone) and neurotrophic factors (BDNF) elicit effects throughout the lifespan, particularly during perinatal and adolescent development. Sex-specific HPA axis stress responsivity can also promote differing vulnerabilities resulting from higher glucocorticoid levels in females and may be related to central CRF regulation. Hormone-independent, genetically programmed sex differences (XX, XY), and disparate life experiences can also play a role in gender-biased vulnerabilities. Together, these factors may predispose females to a higher incidence of stress-related disorders such as affective disorders and drug abuse.
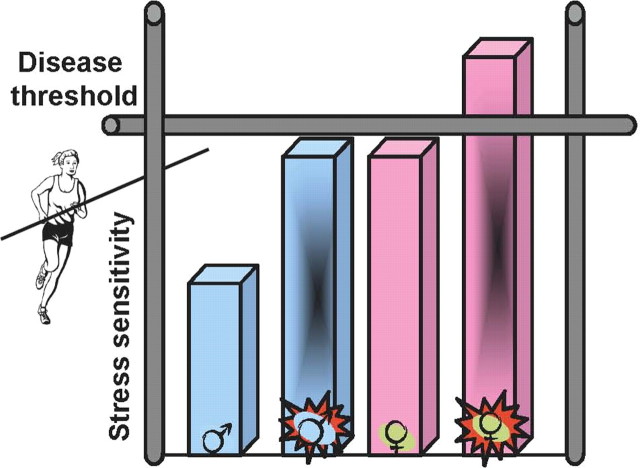
Diagram depicting putative heightened female predisposition toward stress-related disease. The current state of this provocative field suggests that females basally show an exaggerated sensitivity to stress and that if additional dysregulation occurs (such as may result from prenatal stress, maternal PTSD, or a combined impact of stress and gonadal hormones on brain development), this would push females over a “disease threshold” making them more susceptible. If females do in fact show an increased presentation of certain diseases, such as depression and aspects of drug addiction, then examination of those central pathways regulating stress effects and their downstream targets, including critical feedback mechanisms, may provide greater insight into disease susceptibility, treatment, and prevention.
References
-
- Altar CA. Neurotrophins and depression. Trends Pharmacol Sci. 1999;20:59–61. - PubMed
-
- Angold A, Costello EJ, Worthman CM. Puberty and depression: the roles of age, pubertal status and pubertal timing. Psychol Med. 1998;28:51–61. - PubMed
-
- Bale TL. Sensitivity to stress: dysregulation of CRF pathways and disease development. Horm Behav. 2005;48:1–10. - PubMed
-
- Bale TL. Stress sensitivity and the development of affective disorders. Horm Behav. 2006;50:529–533. - PubMed
-
- Bale TL, Contarino A, Smith GW, Chan R, Gold LH, Sawchenko PE, Koob GF, Vale WW, Lee KF. Mice deficient for corticotropin-releasing hormone receptor-2 display anxiety-like behaviour and are hypersensitive to stress. Nat Genet. 2000;24:410–414. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical