

The significance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review
- PMID: 17983433
- PMCID: PMC2228386
- DOI: 10.1111/j.1742-1241.2007.01630.x
The significance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review
Abstract
Objectives: To review studies of patient compliance/persistence with cardiovascular or antidiabetic medication published since the year 2000; to compare the methods used to measure compliance/persistence across studies; to compare reported compliance/persistence rates across therapeutic classes and to assess whether compliance/persistence correlates with clinical outcomes.
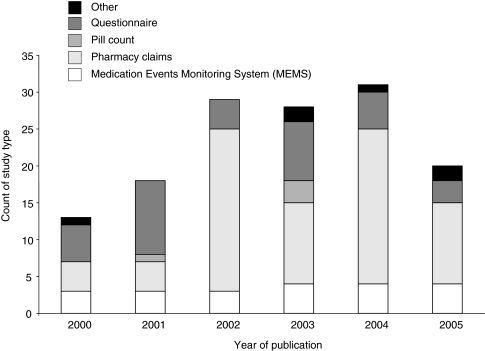
Methods: English language papers published between January 2000 and November 2005 investigating patient compliance/persistence with cardiovascular or antidiabetic medication were identified through searches of the MEDLINE and EMBASE databases. Definitions and measurements of compliance/persistence were compared across therapeutic areas using contingency tables.
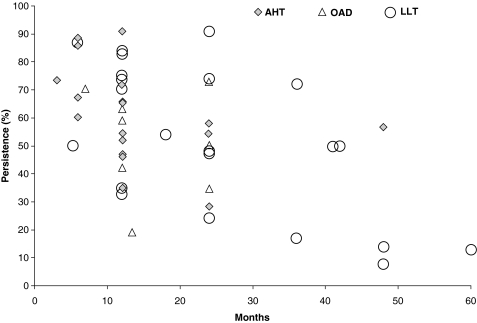
Results: Of the 139 studies analysed, 32% focused on hypertension, 27% on diabetes and 13% on dyslipidaemia. The remainder covered coronary heart disease and cardiovascular disease (CVD) in general. The most frequently reported measure of compliance was the 12-month medication possession ratio (MPR). The overall mean MPR was 72%, and the MPR did not differ significantly between treatment classes (range: 67-76%). The average proportion of patients with an MPR of >80% was 59% overall, 64% for antihypertensives, 58% for oral antidiabetics, 51% for lipid-lowering agents and 69% in studies of multiple treatments, again with no significant difference between treatment classes. The average 12-month persistence rate was 63% and was similar across therapeutic classes. Good compliance had a positive effect on outcome in 73% of the studies examining clinical outcomes.
Conclusions: Non-compliance with cardiovascular and antidiabetic medication is a significant problem, with around 30% of days 'on therapy' not covered by medication and only 59% of patients taking medication for more than 80% of their days 'on therapy' in a year. Good compliance has a positive effect on clinical outcome, suggesting that the management of CVD may be improved by improving patient compliance.
Figures
References
-
- Dzau V, Braunwald E. Resolved and unresolved issues in the prevention and treatment of coronary artery disease: a workshop consensus statement. Am J Heart. 1991;121:1244–63. - PubMed
-
- McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA. 1993;270:2207–12. - PubMed
-
- American Heart Association. Heart Disease and Stroke Statistics – 2006 Update. Dallas, TX: American Heart Association;
-
- Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics – 2006 update. A Report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. 2006;113:e85–151. Epub 11 January 2006. - PubMed
Appendix. Studies included in the systematic review
-
- Abraha I, Montedori A, Stracci F, Rossi M, Romagnoli C. Statin compliance in the Umbrian population. Eur J Clin Pharmacol. 2003;59:659–61. Epub 24 September 2003. - PubMed
-
- Akpa MR, Agomuoh DI, Odia OJ. Drug compliance among hypertensive patients in Port Harcourt, Nigeria. Niger J Med. 2005;14:55–7. - PubMed
-
- Andrejak M, Genes N, Vaur L, Poncelet P, Clerson P, Carre A. Electronic pill-boxes in the evaluation of antihypertensive treatment compliance: comparison of once daily versus twice daily regimen. Am J Hypertens. 2000;13:184–90. - PubMed
-
- Artinian NT, Harden JK, Kronenberg MW, Vander Wal JS, Daher E. Pilot study of a web-based compliance monitoring device for patients with congestive heart failure. Heart Lung. 2003;32:226–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
