

Treatment of myofascial trigger points in common shoulder disorders by physical therapy: a randomized controlled trial [ISRCTN75722066]
- PMID: 17983467
- PMCID: PMC2246010
- DOI: 10.1186/1471-2474-8-107
Treatment of myofascial trigger points in common shoulder disorders by physical therapy: a randomized controlled trial [ISRCTN75722066]
Abstract
Background: Shoulder disorders are a common health problem in western societies. Several treatment protocols have been developed for the clinical management of persons with shoulder pain. However available evidence does not support any protocol as being superior over others. Systematic reviews provide some evidence that certain physical therapy interventions (i.e. supervised exercises and mobilisation) are effective in particular shoulder disorders (i.e. rotator cuff disorders, mixed shoulder disorders and adhesive capsulitis), but there is an ongoing need for high quality trials of physical therapy interventions. Usually, physical therapy consists of active exercises intended to strengthen the shoulder muscles as stabilizers of the glenohumeral joint or perform mobilisations to improve restricted mobility of the glenohumeral or adjacent joints (shoulder girdle). It is generally accepted that a-traumatic shoulder problems are the result of impingement of the subacromial structures, such as the bursa or rotator cuff tendons. Myofascial trigger points (MTrPs) in shoulder muscles may also lead to a complex of symptoms that are often seen in patients diagnosed with subacromial impingement or rotator cuff tendinopathy. Little is known about the treatment of MTrPs in patients with shoulder disorders.The primary aim of this study is to investigate whether physical therapy modalities to inactivate MTrPs can reduce symptoms and improve shoulder function in daily activities in a population of chronic a-traumatic shoulder patients when compared to a wait-and-see strategy. In addition we investigate the recurrence rate during a one-year-follow-up period.
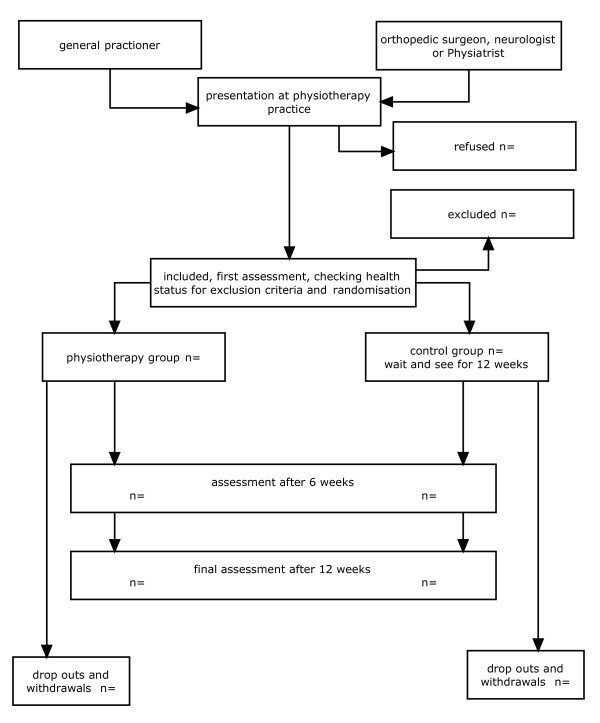
Methods/design: This paper presents the design for a randomized controlled trial to be conducted between September 2007 - September 2008, evaluating the effectiveness of a physical therapy treatment for non-traumatic shoulder complaints. One hundred subjects are included in this study. All subjects have unilateral shoulder pain for at least six months and are referred to a physical therapy practice specialized in musculoskeletal disorders of the neck-, shoulder-, and arm. After the initial assessment patients are randomly assigned to either an intervention group or a control-group (wait and see). The primary outcome measure is the overall score of the Dutch language version of the DASH (Disabilities of Arm, Shoulder and Hand) questionnaire.
Discussion: Since there is only little evidence for the efficacy of physical therapy interventions in certain shoulder disorders, there is a need for further research. We found only a few studies examining the efficacy of MTrP therapy for shoulder disorders. Therefore we will perform a randomised clinical trial of the effect of physical therapy interventions aimed to inactivate MTrPs, on pain and impairment in shoulder function in a population of chronic a-traumatic shoulder patients. We opted for an intervention strategy that best reflects daily practice. Manual high velocity thrust techniques and dry-needling are excluded. Because in most physical therapy interventions, blinding of the patient and the therapist is not possible, we will perform a randomised, controlled and observer-blinded study.
Trial registration: This randomized clinical trial is registered at current controlled trials ISRCTN75722066.
References
-
- Bergman GJD. Manipulative therapy for shoulder complaints in general practice. University of Groningen, The Netherlands; 2005.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
