

Multiple treatment comparisons in epilepsy monotherapy trials
- PMID: 17983480
- PMCID: PMC2194733
- DOI: 10.1186/1745-6215-8-34
Multiple treatment comparisons in epilepsy monotherapy trials
Abstract
Background: The choice of antiepileptic drug for an individual should be based upon the highest quality evidence regarding potential benefits and harms of the available treatments. Systematic reviews and meta-analysis of randomised controlled trials should be a major source of evidence supporting this decision making process. We summarise all available individual patient data evidence from randomised controlled trials that compared at least two out of eight antiepileptic drugs given as monotherapy.
Methods: Multiple treatment comparisons from epilepsy monotherapy trials were synthesized in a single stratified Cox regression model adjusted for treatment by epilepsy type interactions and making use of direct and indirect evidence. Primary outcomes were time to treatment failure and time to 12 month remission from seizures. A secondary outcome was time to first seizure.
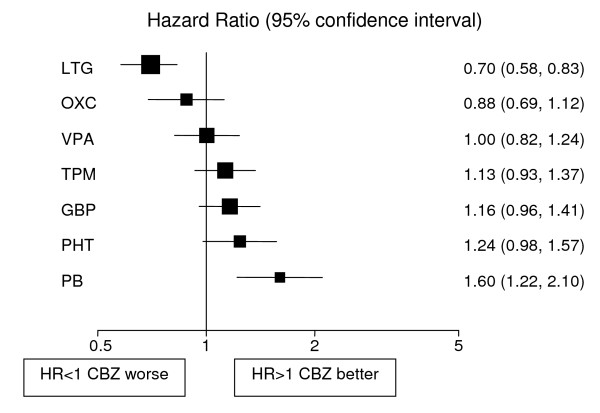
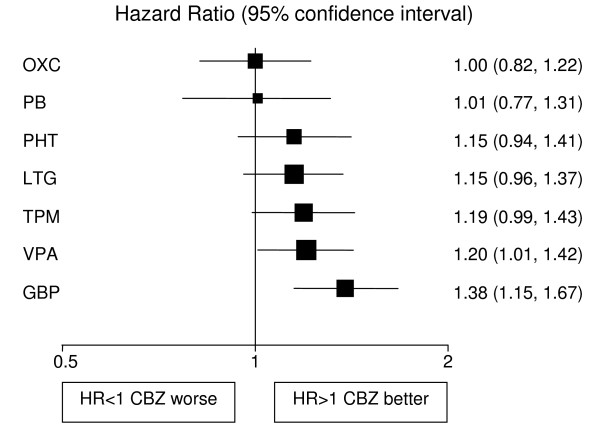
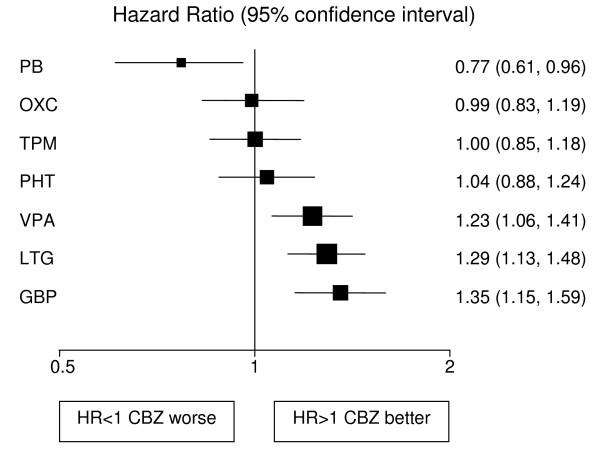
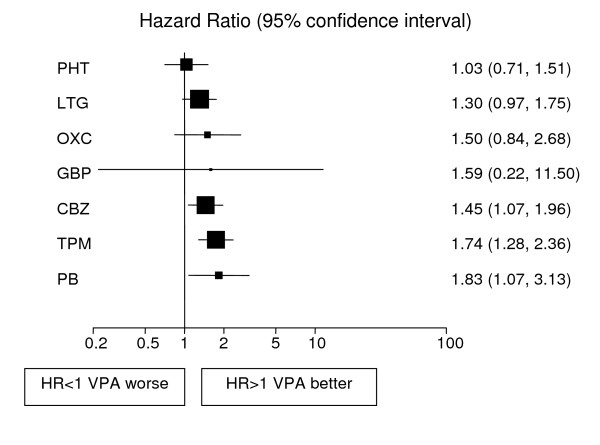
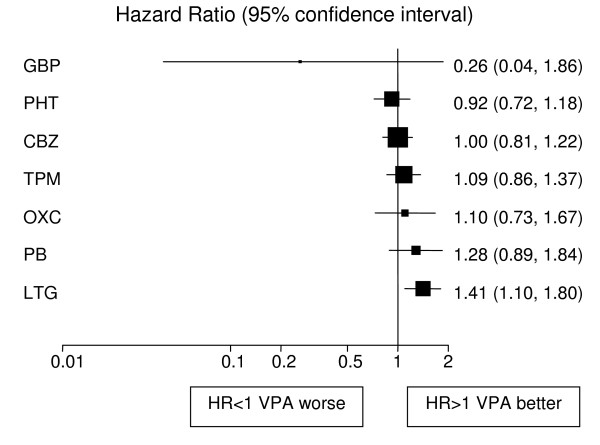
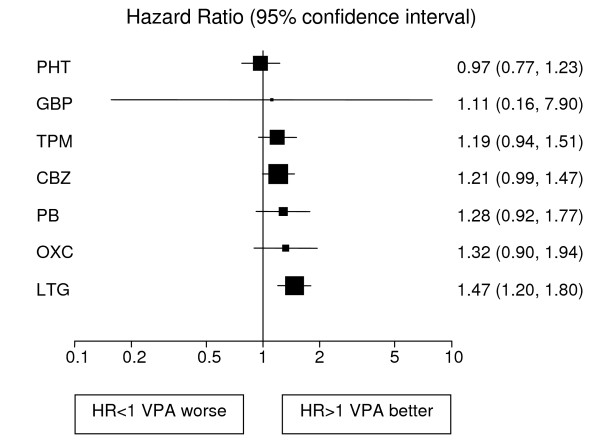
Results: Individual patient data for 6418 patients from 20 randomised trials comparing eight antiepileptic drugs were synthesized. For partial onset seizures (4628 (72%) patients), lamotrigine, carbamazepine and oxcarbazepine provide the best combination of seizure control and treatment failure. Lamotrigine is clinically superior to all other drugs for treatment failure but estimates suggest a disadvantage compared to carbamazepine for time to 12 month remission [Hazard Ratio (95% Confidence Interval) = 0.87(0.73 to 1.04)] and time to first seizure [1.29(1.13 to 1.48)]. Phenobarbitone may delay time to first seizure [0.77(0.61 to 0.96)] but at the expense of increased treatment failure [1.60(1.22 to 2.10)]. For generalized onset tonic clonic seizures (1790 (28%) patients) estimates suggest valproate or phenytoin may provide the best combination of seizure control and treatment failure but some uncertainty remains about the relative effectiveness of other drugs.
Conclusion: For patients with partial onset seizures, results favour carbamazepine, oxcarbazepine and lamotrigine. For generalized onset tonic clonic seizures, results favour valproate and phenytoin.
Figures
References
-
- Hauser WA, Hesdorffer DC. Epilepsy: frequency, causes and consequences. New York: Demos Publications; 1990.
-
- The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care. London: National Institute for Clinical Excellence; 2004. Clinical Guideline 20.
-
- French JA, Kanner AM, Bautista J, Abou-Khalil B, Browne T, Harden CL, Theodore WH, Bazil C, Stern J, Schachter SC, Bergen D, Hirtz D, Montouris GD, Nespeca M, Gidal B, Marks WJ, Jr, Turk WR, Fischer JH, Bourgeois B, Wilner A, Faught RE, Jr, Sachdeo RC, Beydoun A, Glauser TA. Efficacy and tolerability of the new antiepileptic drugs I : treatment of new onset epilepsy: report of the therapeutics and technology assessment subcommittee and quality standards subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology. 2004;62:1252–60. - PubMed
LinkOut - more resources
Full Text Sources
