

Hepatitis B virus e antigen loss during adefovir dipivoxil therapy is associated with enhanced virus-specific CD4+ T-cell reactivity
- PMID: 17984230
- PMCID: PMC2223883
- DOI: 10.1128/AAC.00467-07
Hepatitis B virus e antigen loss during adefovir dipivoxil therapy is associated with enhanced virus-specific CD4+ T-cell reactivity
Abstract
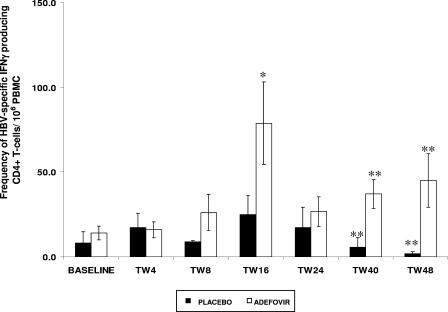
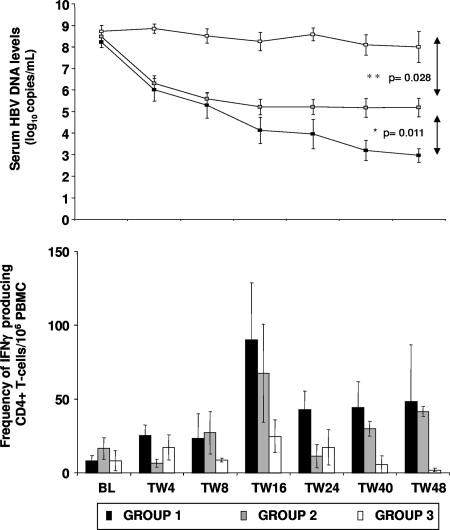
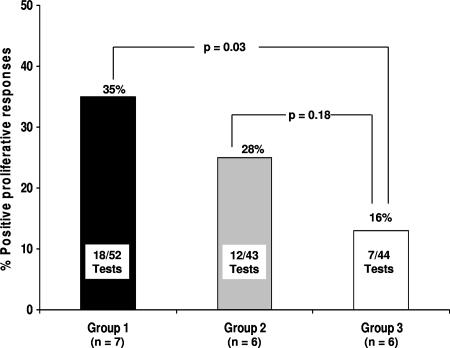
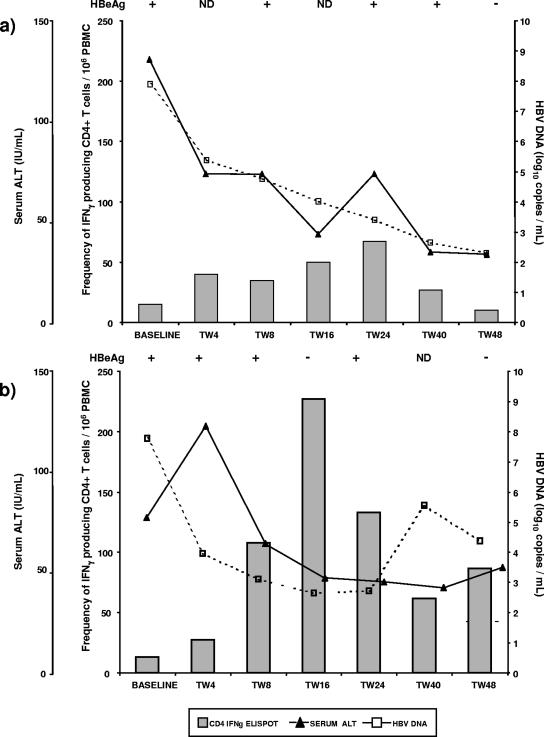
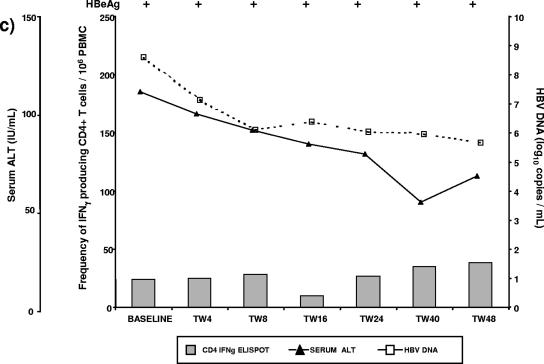
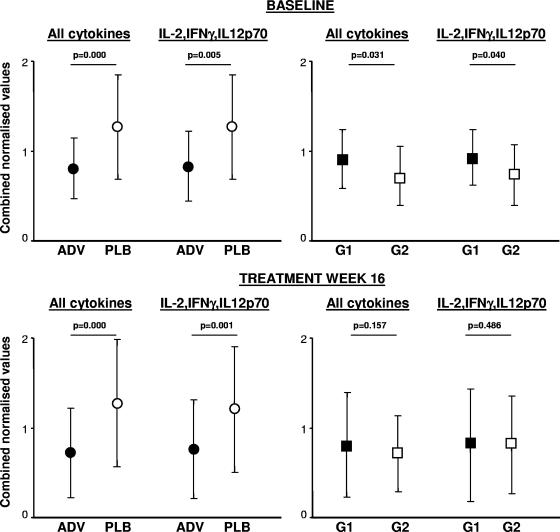
Weak T-cell reactivity to hepatitis B virus (HBV) is thought to be the dominant cause for chronic HBV infection. Treatment with adefovir dipivoxil (ADV) increases the rate of HBV e antigen (HBeAg) loss; however, the immune mechanisms associated with this treatment response are not understood. Serial analysis of HBV-specific CD4+ T-cell reactivity was performed during 48 weeks of therapy with ADV and correlated with treatment outcome for 19 HBeAg-positive patients receiving ADV (n = 13) or the placebo (n = 6). We tested T-cell reactivity to HBV at seven protocol time points by proliferation, cytokine production, and enzyme-linked immunospot assays. A panel of serum cytokines was quantitated by cytokine bead array. ADV-treated patients showed increased CD4+ T-cell responses to HBV and lower serum levels of cytokines compared to those of placebo-treated patients. Enhanced CD4+ T-cell reactivity to HBV, which peaked at treatment week 16, was confined to a subgroup of ADV-treated patients who achieved greater viral suppression (5.3 +/- 0.3 log(10) copies/ml [mean +/- standard error of the mean {SEM}] serum HBV DNA reduction from baseline) and HBeAg loss, but not to ADV-treated patients with moderate (3.4 +/- 0.2 log(10) copies/ml [mean +/- SEM]) viremia reduction who remained HBeAg positive or to patients receiving the placebo. In conclusion, T-cell reactivity to HBV increases in a proportion of ADV-treated patients and is associated with greater suppression of HBV replication and HBeAg loss.
Figures
References
-
- Boni, C., A. Penna, A. Bertoletti, V. Lamonaca, I. Rapti, G. Missale, M. Pilli, S. Urbani, A. Cavalli, S. Cerioni, R. Panebianco, J. Jenkins, and C. Ferrari. 2003. Transient restoration of anti-viral T cell responses induced by lamivudine therapy in chronic hepatitis B. J. Hepatol. 39:595-605. - PubMed
-
- Chisari, F. V., and C. Ferrari. 1995. Hepatitis B virus immunopathogenesis. Annu. Rev. Immunol. 13:29-60. - PubMed
-
- de Franchis, R., A. Hadengue, G. Lau, D. Lavanchy, A. Lok, N. McIntyre, A. Mele, G. Paumgartner, A. Pietrangelo, J. Rodes, W. Rosenberg, D. Valla, and the EASL Jury. 2003. EASL Consensus Conference on Hepatitis B: consensus statement. J. Hepatol. 39(Suppl. 1):S3-S25. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
