

Morphologic features of the amygdala and hippocampus in children and adults with Tourette syndrome
- PMID: 17984397
- PMCID: PMC2291296
- DOI: 10.1001/archpsyc.64.11.1281
Morphologic features of the amygdala and hippocampus in children and adults with Tourette syndrome
Abstract
Context: Limbic portions of cortical-subcortical circuits are likely involved in the pathogenesis of Tourette syndrome (TS). They are anatomically, developmentally, neurochemically, and functionally related to the basal ganglia, and the basal ganglia are thought to produce the symptoms of tics, obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder that commonly affect persons with TS.
Objective: To study the morphologic features of the hippocampus and amygdala in children and adults with TS.
Design: A cross-sectional, case-control study using anatomical magnetic resonance imaging.
Setting: University research center.
Participants: A total of 282 individuals (154 patients with TS and 128 controls) aged 6 to 63 years.
Main outcome measures: Volumes and measures of surface morphologic features of the hippocampus and amygdala.
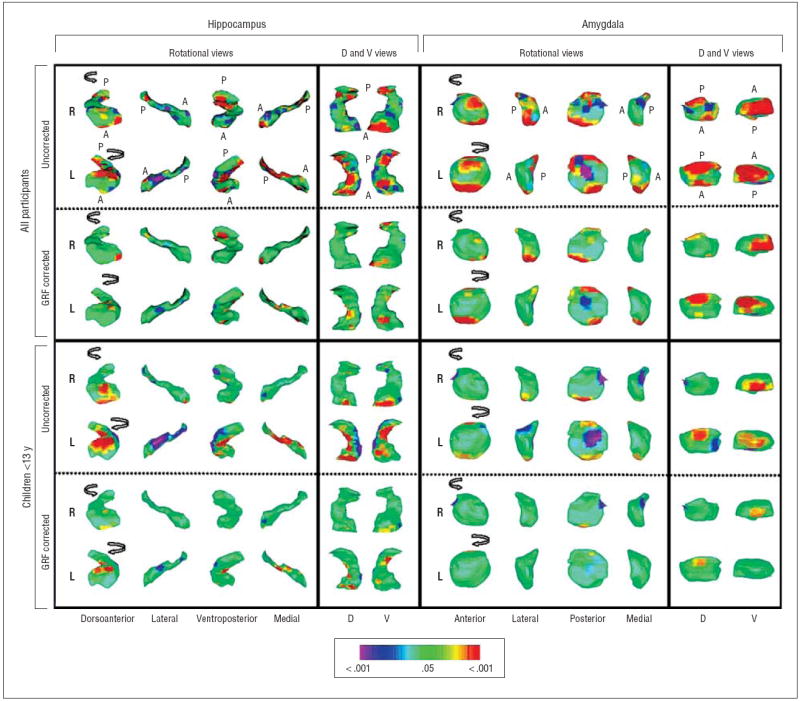
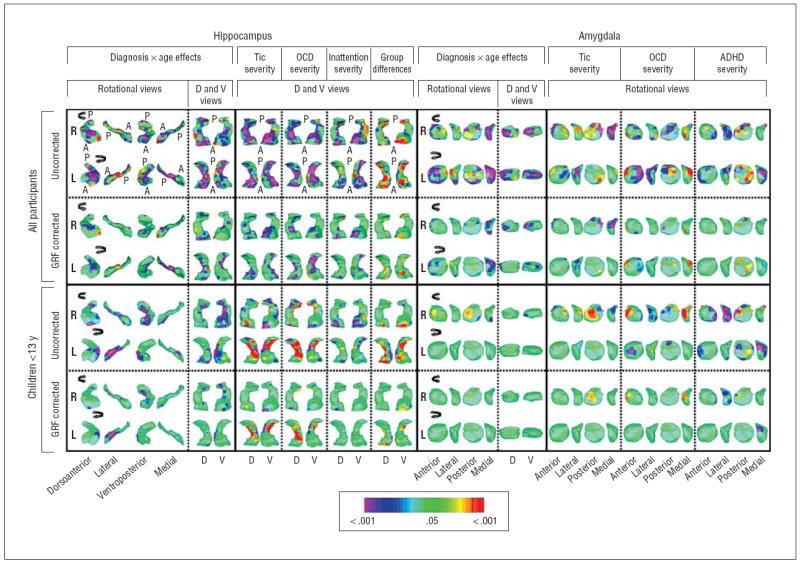
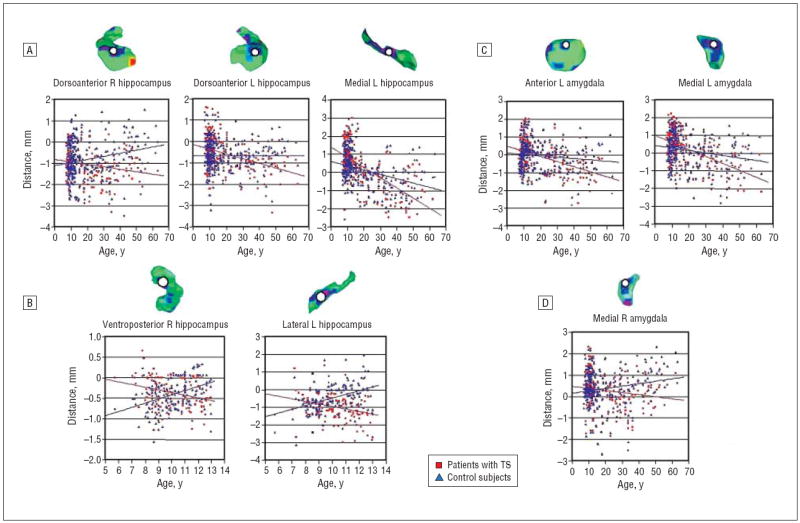
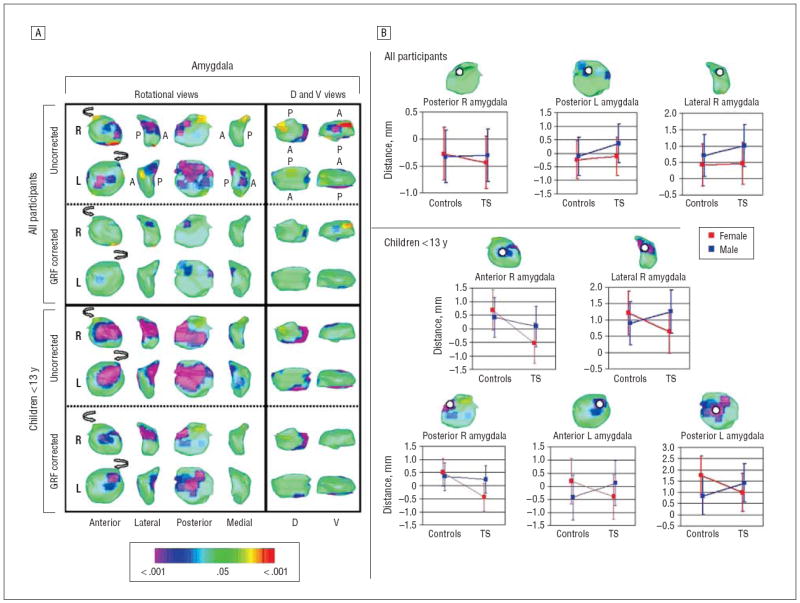
Results: The overall volumes of the hippocampus and amygdala were significantly larger in the TS group. Surface analyses suggested that the increased volumes in the TS group derived primarily from the head and medial surface of the hippocampus (over the length of the dentate gyrus) and the dorsal and ventral surfaces of the amygdala (over its basolateral and central nuclei). Volumes of these subregions declined with age in the TS group but not in controls, so the subregions were significantly larger in children with TS but significantly smaller in adults with TS than in their control counterparts. In children and adults, volumes in these subregions correlated inversely with the severity of tic, obsessive-compulsive disorder, and attention-deficit/hyperactivity disorder symptoms, suggesting that enlargement of the subregions may have a compensatory and neuromodulatory effect on tic-related symptoms.
Conclusion: These findings are consistent with the known plasticity of the dentate gyrus and with findings from previous imaging studies suggesting the presence of failed compensatory plasticity in adults with TS who have not experienced the usual decline in symptoms during adolescence.
Figures
References
-
- Pauls DL. An update on the genetics of Gilles de la Tourette syndrome. J Psychosom Res. 2003;55(1):7–12. - PubMed
-
- Peterson BS, Staib L, Scahill L, Zhang H, Anderson C, Leckman JF, Cohen DJ, Gore JC, Albert J, Webster R. Regional brain and ventricular volumes in Tourette syndrome. Arch Gen Psychiatry. 2001;58(5):427–440. - PubMed
-
- Peterson BS, Thomas P, Kane MJ, Scahill L, Zhang H, Bronen R, King RA, Leckman JF, Staib L. Basal ganglia volumes in patients with Gilles de la Tourette syndrome. Arch Gen Psychiatry. 2003;60(4):415–424. - PubMed
-
- Parent A, Hazrati LN. Functional anatomy of the basal ganglia, I: the corticobasal ganglia-thalamo-cortical loop. Brain Res Brain Res Rev. 1995;20(1):91–127. - PubMed
-
- Fudge JL, Kunishio K, Walsh P, Richard C, Haber SN. Amygdaloid projections to ventromedial striatal subterritories in the primate. Neuroscience. 2002;110(2):257–275. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
