

Prediction of health professionals' intention to screen for decisional conflict in clinical practice
- PMID: 17986073
- PMCID: PMC5060414
- DOI: 10.1111/j.1369-7625.2007.00465.x
Prediction of health professionals' intention to screen for decisional conflict in clinical practice
Abstract
Objective: To identify the determinants of the intention of physicians to screen for decisional conflict in clinical practice.
Background: Screening for decisional conflict is one of the key competencies when educating health professionals about shared decision making. Theory-based knowledge about variables predicting their intention to screen for decisional conflict in clinical practice would help design effective implementation interventions in this area.
Design: Data of two cross-sectional surveys embedded within a large implementation study of the Ottawa Decision Support Framework (ODSF) in primary care.
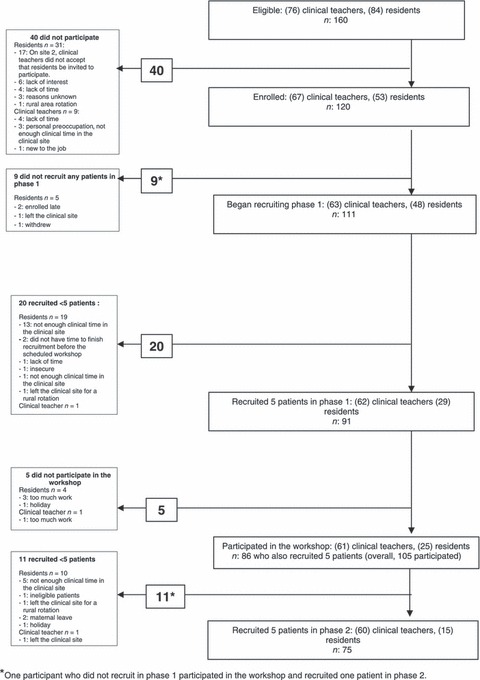
Setting and participants: In total, 122 health professionals from five family practice teaching units.
Methods: Intention to screen for decisional conflict in clinical practice was defined as the intention to use the clinical version of the Decisional Conflict Scale (DCS) with patients at the end of the clinical encounter. It was assessed at the entry and the exit from this study. Both intentions were entered as a dependent variable in multivariate analyses.
Main results: At entry, the intention was influenced by: attitude (P < 0.001), subjective norm (P < 0.001), perceived behavioural control (P < 0.001) and clinical site (P < 0.05). On exit, it was influenced by: subjective norm (P < 0.001), perceived behavioural control (P < 0.001), clinical site (P < 0.05), international Continuing Medical Education (CME) (P < 0.05), other diplomas (P < 0.05) and intervention (P < 0.05). In post hoc analyses, there was a statistically significant difference between entry and exit in the impact of the level of exposure to the multifaceted implementation intervention on the intention (P = 0.003).
Conclusions: Variables predicting the intention of health professionals to screen for decisional conflict in clinical practice using the DCS change over time suggesting that effective implementation interventions in this area will need to be modified longitudinally.
References
-
- Hibbard JH. Engaging health care consumers to improve the quality of care. Medical Care, 2003; 41: I61–I70. - PubMed
-
- Towle A, Godolphin W. Education and training of health care professionals In: Edwards A, Elwyn G. (eds) Evidence‐Based Patient Choice Inevitable or Impossible? Oxford: Oxford University Press, 2001: 245–270.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
