

Tranexamic acid attenuates inflammatory response in cardiopulmonary bypass surgery through blockade of fibrinolysis: a case control study followed by a randomized double-blind controlled trial
- PMID: 17988379
- PMCID: PMC2246206
- DOI: 10.1186/cc6173
Tranexamic acid attenuates inflammatory response in cardiopulmonary bypass surgery through blockade of fibrinolysis: a case control study followed by a randomized double-blind controlled trial
Abstract
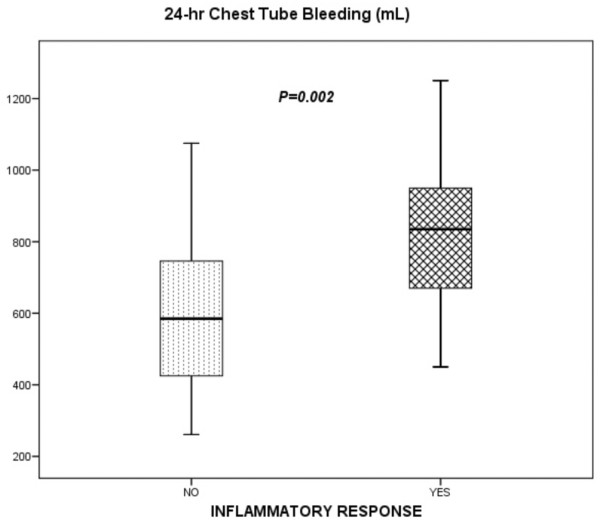
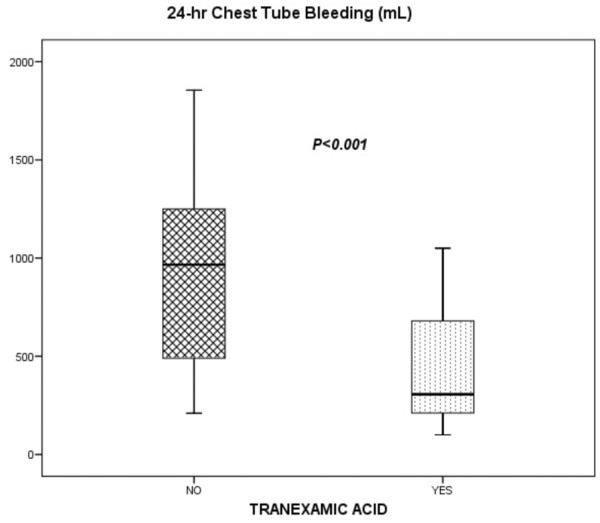
Introduction: Extracorporeal circulation induces hemostatic alterations that lead to inflammatory response (IR) and postoperative bleeding. Tranexamic acid (TA) reduces fibrinolysis and blood loss after cardiopulmonary bypass (CPB). However, its effects on IR and vasoplegic shock (VS) are not well known and elucidating these effects was the main objective of this study.
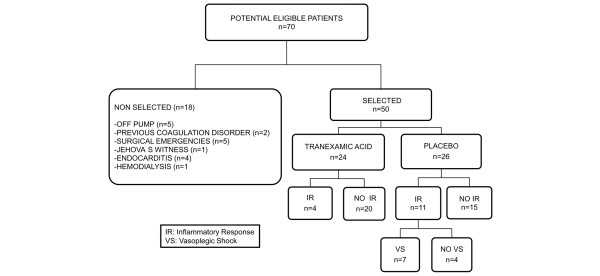
Methods: A case control study was carried out to determine factors associated with IR after CPB. Patients undergoing elective CPB surgery were randomly assigned to receive 2 g of TA or placebo (0.9% saline) before and after intervention. We performed an intention-to-treat analysis, comparing the incidence of IR and VS. We also analyzed several biological parameters related to inflammation, coagulation, and fibrinolysis systems. We used SPSS version 12.2 for statistical purposes.
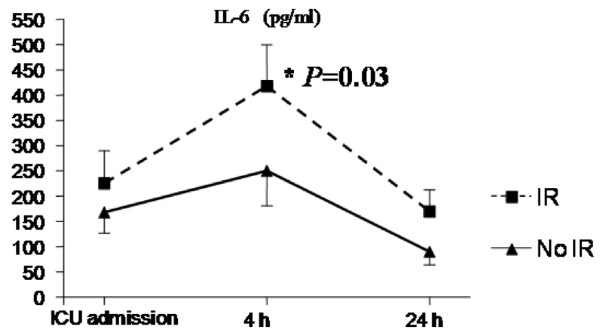
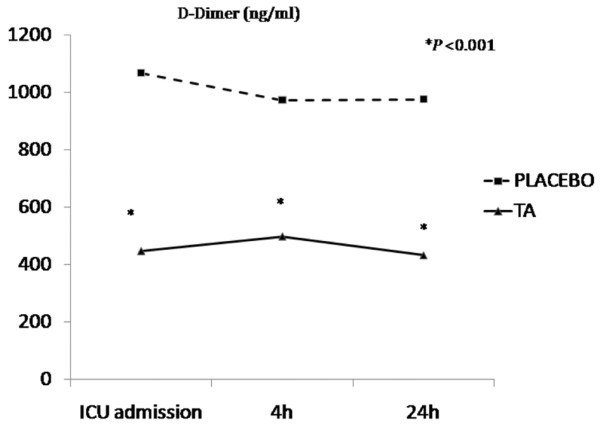
Results: In the case control study, 165 patients were studied, 20.6% fulfilled IR criteria, and the use of TA proved to be an independent protective variable (odds ratio 0.38, 95% confidence interval 0.18 to 0.81; P < 0.01). The clinical trial was interrupted. Fifty patients were randomly assigned to receive TA (24) or placebo (26). Incidence of IR was 17% in the TA group versus 42% in the placebo group (P = 0.047). In the TA group, we observed a significant reduction in the incidence of VS (P = 0.003), the use of norepinephrine (P = 0.029), and time on mechanical ventilation (P = 0.018). These patients showed significantly lower D-dimer, plasminogen activator inhibitor 1, and creatine-kinase levels and a trend toward lower levels of soluble tumor necrosis factor receptor and interleukin-6 within the first 24 hours after CPB.
Conclusion: The use of TA attenuates the development of IR and VS after CPB.
Figures
Comment in
-
An anti-inflammatory role for tranexamic acid in cardiac surgery?Crit Care. 2008;12(1):105. doi: 10.1186/cc6210. Epub 2008 Jan 16. Crit Care. 2008. PMID: 18254939 Free PMC article.
References
-
- Taneja R, Yared JP, Hammel J, O'Connor MS, Insler S, Starr NJ. Hyperdynamic circulation following cardiopulmonary bypass predisposes to postoperative bleeding. Critical Care. 2001;5(Suppl 1):P110. (2 March 2001)
-
- Greilich PE, Brouse CF, Whitten CW, Chi L, Dimaio JM, Jessen ME. Antifibrinolytic therapy during cardiopulmonary bypass reduces proinflammatory cytokine levels: a randomized, double-blind, placebo-controlled study of epsilon-aminocaproic acid and aprotinin. J Thorac Cardiovasc Surg. 2003;126:1498–1503. doi: 10.1016/S0022-5223(03)00946-2. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
