

Trends in end-of-life ICU use among older adults with advanced lung cancer
- PMID: 17989164
- PMCID: PMC4034445
- DOI: 10.1378/chest.07-1007
Trends in end-of-life ICU use among older adults with advanced lung cancer
Abstract
Background: There is increasing concern about the appropriateness of intensive medical care near the end of life in ICUs throughout the United States. As a result of hospice expansion in the 1990s, we hypothesized that ICU use decreased over time in older adults with advanced lung cancer.
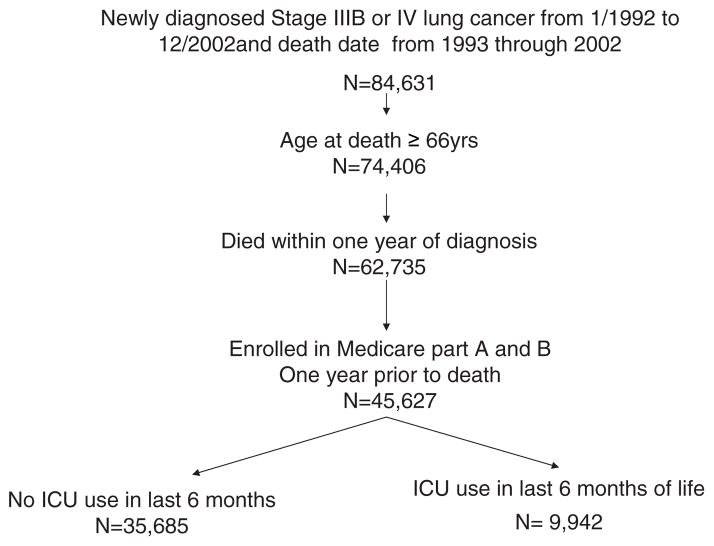
Methods: Retrospective analysis using the linked Surveillance, Epidemiology and End Results Medicare database. There were 45,627 Medicare beneficiaries > or = 66 years of age with confirmed stage IIIB or IV lung cancer between January 1, 1992, and December 31, 2002, who died within a year of their cancer diagnosis from 1993 through 2002.
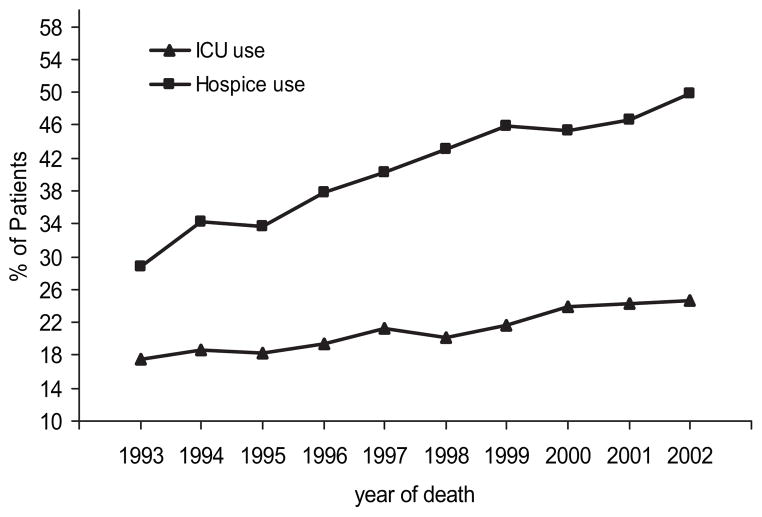
Results: ICU use in the last 6 months of life increased from 17.5% in 1993 to 24.7% in 2002 (p < 0.001). After adjusting for patient characteristics, there was a 6.6% annual increase in ICU use from 1993 to 2002. During the same period, hospice use had risen from 28.8 to 49.9% (p < 0.001). A total of 6.2% of patients received both end-of-life ICU care and hospice care, a percentage that increased over time. The total health-care cost for Medicare fee-for-service patients during last 6 months was $40,929 for ICU users and $27,160 for non-ICU users (p < 0.001).
Conclusion: Despite increasing hospice use, ICU utilization among older adults dying with advanced lung cancer continued to rise in the United States during the 1990s.
Conflict of interest statement
The authors have reported to the ACCP that no significant conflicts of interest exist with any companies/organizations whose products or services may be discussed in this article.
Figures
References
-
- Spiro SS, Silvestri GA. One hundred years of lung cancer. Am J Respir Crit Care Med. 2005;172:523–529. - PubMed
-
- Ries LAG, Melbert D, Krapcho M, et al., editors. [Accessed November 14, 2007];SEER cancer statistics review, 1975–2004. Available at: http://seer.cancer.gov/csr/1975_2004/
-
- Griffin JP, Nelson JE, Koch KA, et al. End-of-life care in patients with lung cancer. Chest. 2003;123:312S–331S. - PubMed
-
- Angus DC, Barnato AE, Linde-Zwirble WT, et al. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
