

Prevalence and risk factors for aspirin and clopidogrel resistance in cerebrovascular stenting
- PMID: 17989373
- PMCID: PMC8118987
- DOI: 10.3174/ajnr.A0818
Prevalence and risk factors for aspirin and clopidogrel resistance in cerebrovascular stenting
Abstract
Background and purpose: The prevalence of antiplatelet drug resistance among patients who undergo cerebrovascular stent placement is unknown. We aimed to assess the feasibility of monitoring antiplatelet drug effects in a single-center cohort undergoing cerebrovascular stent placement.
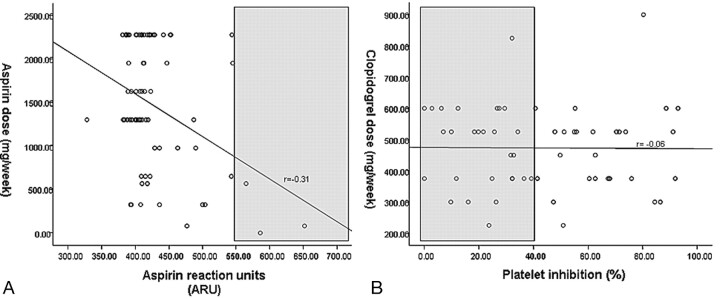
Materials and methods: We prospectively collected medical, laboratory, and radiographic data on patients who underwent cerebrovascular stent placement. We used the rapid platelet function assay-aspirin (RPFA-ASA) to calculate aspirin reaction units (ARU) and the P2Y12 assay to calculate P2Y12 reaction units and percentage platelet inhibition. Aspirin resistance was defined as ARU > 550, whereas clopidogrel resistance was defined as percentage platelet inhibition < 40%.
Results: Among 76 patients, stent indications were the following: wide-neck aneurysm (57, 75.0%), symptomatic intracranial stenosis (12, 15.7%), carotid stenosis (5, 6.6%), and vertebral stenosis (2, 2.6%). For aspirin, the median dosage per week was 1300 mg and median ARU was 410. Among 71 patients on aspirin, 3 patients (4.2%) were resistant; there was a significant inverse correlation between aspirin dose and ARU (r = -0.31, P = .01). Among 55 patients on clopidogrel, the median dosage per week was 525 mg with a mean platelet inhibition of 43.2%. Twenty-eight patients (51.9%) were clopidogrel-resistant. In a multivariable linear regression model, age older than 55 years (b = -16.3, P = .020) and diabetes (b = -26.8, P = .015) were inversely related to percentage platelet inhibition.
Conclusions: Using point-of-care tests, we found that aspirin resistance is relatively uncommon, whereas clopidogrel resistance occurred in half of patients undergoing cerebrovascular stent placement. Further studies should focus on ideal doses, timing, and duration of antiplatelet therapy for cerebrovascular stent placement.
Figures
References
-
- Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update 2001 Guidelines for Percutaneous Coronary Intervention). Circulation 2006;113:e166–286 - PubMed
-
- SSYLVIA Study Investigators. Stenting of Symptomatic Atherosclerotic Lesions in the Vertebral or Intracranial Arteries (SSYLVIA): study results. Stroke 2004;35:1388–92. Epub 2004 Apr 22 - PubMed
-
- Fiorella D, Levy EI, Turk AS, et al. US multicenter experience with the Wingspan stent system for the treatment of intracranial atheromatous disease: periprocedural results. Stroke 2007;38:881–87. Epub 2007 Feb 8 - PubMed
-
- Henkes H, Miloslavski E, Lowens S, et al. Treatment of intracranial atherosclerotic stenoses with balloon dilatation and self-expanding stent deployment (WingSpan). Neuroradiology 2005;47:222–28 - PubMed
-
- Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, et al. Identification of low responders to a 300-mg clopidogrel loading dose in patients undergoing coronary stenting. Thromb Res 2005;115:101–08 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources